



Amarin - The Science Of Lipid Therapy (Seite 26)
eröffnet am 03.01.14 20:10:32 von
neuester Beitrag 04.04.24 15:47:54 von
neuester Beitrag 04.04.24 15:47:54 von
Beiträge: 1.840
ID: 1.190.027
ID: 1.190.027
Aufrufe heute: 0
Gesamt: 156.356
Gesamt: 156.356
Aktive User: 0
ISIN: US0231112063 · WKN: A0NBNG · Symbol: AMRN
0,8593
USD
-1,43 %
-0,0125 USD
Letzter Kurs 02:00:00 Nasdaq
Neuigkeiten
15.04.24 · globenewswire |
Amarin Highlights Key Data Providing Mechanistic Insights into Eicosapentaenoic Acid (EPA) at ACC.24 08.04.24 · globenewswire |
06.04.24 · globenewswire |
03.04.24 · globenewswire |
Werte aus der Branche Pharmaindustrie
| Wertpapier | Kurs | Perf. % |
|---|---|---|
| 3,5800 | +922,86 | |
| 0,5400 | +38,46 | |
| 1,9900 | +32,67 | |
| 5,4000 | +27,06 | |
| 1,8250 | +25,86 |
| Wertpapier | Kurs | Perf. % |
|---|---|---|
| 5,0100 | -26,54 | |
| 14,510 | -32,32 | |
| 3,6400 | -38,62 | |
| 0,5660 | -40,42 | |
| 84,75 | -74,50 |
Beitrag zu dieser Diskussion schreiben
Antwort auf Beitrag Nr.: 68.567.716 von bernie55 am 21.06.21 12:12:06 QUICKI- Info vom SCOTUS:
Cert denied. 👎
https://www.supremecourt.gov/search.aspx?filename=/docket/do…
https://www.supremecourt.gov/search.aspx?filename=/docket/do…
Cert denied. 👎
https://www.supremecourt.gov/search.aspx?filename=/docket/do…
https://www.supremecourt.gov/search.aspx?filename=/docket/do…
HEUTE wird es sich zeigen, wie der SCOTUS entscheiden wird.
Welche Leitlinien wird der SCOTUS formulieren ?
Wird das "Du-Desaster" Bestand haben ?
Wird der SCOTUS ein zukunftsweisendes Urteil ( auch im Hinblick auf Gültigkeitserklärungen von Patenten) abgeben ?
Wird der SCOTUS die Entscheidung verschieben ?
Um 9.30 Uhr (EST) = 15.30 Uhr ( MEZ) wissen wir es !!!
Welche Leitlinien wird der SCOTUS formulieren ?
Wird das "Du-Desaster" Bestand haben ?
Wird der SCOTUS ein zukunftsweisendes Urteil ( auch im Hinblick auf Gültigkeitserklärungen von Patenten) abgeben ?
Wird der SCOTUS die Entscheidung verschieben ?
Um 9.30 Uhr (EST) = 15.30 Uhr ( MEZ) wissen wir es !!!
Amarin Co. ADR Aktie......WKN: A0NBNG....... ISIN: US0231112063
Weitere Einblicke in den Wirkmechanismus von Icosapent Ethyl und seine einzigartige Form der Eicosapentaensäure (EPA) präsentiert auf dem Kongress der European Atherosclerosis Society (EAS) 2021
[https://finance.yahoo.com/news/further-insights-mechanism-ac…
Weitere Einblicke in den Wirkmechanismus von Icosapent Ethyl und seine einzigartige Form der Eicosapentaensäure (EPA) präsentiert auf dem Kongress der European Atherosclerosis Society (EAS) 2021
[https://finance.yahoo.com/news/further-insights-mechanism-ac…
Antwort auf Beitrag Nr.: 68.533.725 von Rastelly am 17.06.21 09:40:21
Die AMRN-Aktionäre können alle NUR hoffen, dass die Gerechtigkeit siegen wird, auch wenn, wie ich bereits geschrieben habe, Amarins Gewinn-Chancen - statistisch gesehen - beim SCOTUS als sehr gering einzuschätzen sind.
ABER!!!
Die Hoffnung stirbt zuletzt.
Grüße
bernie55
Zitat von Rastelly: @bernie55
du machst das mit dem Einstellen der Beiträgen super,DANKE für dein Lob - gern geschehen.
Aus Erfahrung mit anderen Rechtsstreitigkeiten in den USA (erinnerst du dich an Rambus ??? ) bin ich nicht so positiv gestimmt , aber natürlich mit der Hoffnung!!
Es wird in die Länge gezogen - eben juristisch aufgearbeitet, für Aktionäre nicht vorteilhaft.
Natürlich kann und weiss ich als Aktionär mit dem Zeitfaktor zu Leben, die Ungewissheit frisst!!
Noch bin ich investiert, wie lange noch???
Allerdings sind wir schon fast wieder vom Aktienkurs in den 2018 Jahren.
Nur die Zukunft zählt und damit die Aussicht und Phantasie, das Urteil !!??
Gruss RS

Die AMRN-Aktionäre können alle NUR hoffen, dass die Gerechtigkeit siegen wird, auch wenn, wie ich bereits geschrieben habe, Amarins Gewinn-Chancen - statistisch gesehen - beim SCOTUS als sehr gering einzuschätzen sind.
ABER!!!
Die Hoffnung stirbt zuletzt.
Grüße
bernie55

@berni55
du machst das mit dem Einstellen der Beiträgen super, 👍.
Aus Erfahrung mit anderen Rechtsstreitigkeiten in den USA (erinnerst du dich an Rambus ??? ) bin ich nicht so positiv gestimmt , aber natürlich mit der Hoffnung!!
Es wird in die Länge gezogen - eben juristisch aufgearbeitet, für Aktionäre nicht vorteilhaft.
Natürlich kann und weiss ich als Aktionär mit dem Zeitfaktor zu Leben, die Ungewissheit frisst!!
Noch bin ich investiert, wie lange noch???
Allerdings sind wir schon fast wieder vom Aktienkurs in den 2018 Jahren.
Nur die Zukunft zählt und damit die Aussicht und Phantasie, das Urteil !!??
Gruss RS😎
du machst das mit dem Einstellen der Beiträgen super, 👍.
Aus Erfahrung mit anderen Rechtsstreitigkeiten in den USA (erinnerst du dich an Rambus ??? ) bin ich nicht so positiv gestimmt , aber natürlich mit der Hoffnung!!
Es wird in die Länge gezogen - eben juristisch aufgearbeitet, für Aktionäre nicht vorteilhaft.
Natürlich kann und weiss ich als Aktionär mit dem Zeitfaktor zu Leben, die Ungewissheit frisst!!
Noch bin ich investiert, wie lange noch???
Allerdings sind wir schon fast wieder vom Aktienkurs in den 2018 Jahren.
Nur die Zukunft zählt und damit die Aussicht und Phantasie, das Urteil !!??
Gruss RS😎
Trading Spotlight
Heute , am 17.Juni , wird der SCOTUS ( Supreme Court of the USA) zusammenkommen

Am 21 Juni wird der SCOTUS dann sein Urteil bzgl. der Amarinklage bekanntgeben.
Hier noch einmal kurz zusammengefasst - die "Forderung" von Amarin an den SCOTUS :
Das Gericht sollte eine umfassende Überprüfung gewähren, um den Fehler in der Rechtssprechung des Bundesgerichtshofs zu korrigieren. Zumindest aber das Urteil aufzuheben und an den Bundesgerichtshof zurückzuweisen mit der Anweisung, nach dem Aspekt des "Grahamprinzips" juristisch vorzugehen bzw. zu verfahren.
Welche Entscheidung wird/könnte der SCOTUS fällen ?
Wie wird der Ausgang des Urteils Amarins Zukunft beeinflussen ?
Statistisch gesehen sind Amarins Gewinn-Chancen beim SCOTUS als sehr gering einzuschätzen.
MÖGLICHE SCOTUS-ENTSCHEIDUNGEN:
- Aufhebung des Urteils und Entscheidung für Amarin nach Anwendung des Grahamprinzips.👍
Der Supreme Court könnte rein theoretisch über die "Offensichtlichkeit" entscheiden. Ob er sich aber so intensiv mit dem Fall beschäftigen wird, um eine Entscheidung zu treffen, bezweifel ich stark, da u.a wissenschaftlich-technische Aspekte eine wichtige Rolle spielen und Aussagen von Experten von großer Bedeutung sein werden.
- Annahme der Amarin-Klage zur Verhandlung.👍
Eine Annahme des Falls durch den Supreme Court, um dann eine endgültige Entscheidung in einer späteren Verhandlung bzgl. der "Offensichtlichkeit" zu fällen - dieser juristische Schritt würde tendenziell bedeuten, dass große Zweifel am vorherigen Urteil bestünden.
- Aufhebung des Urteils und Rückverweisung an den Bundesgerichtshof👍
Ausgestattet mit deutlicher Kritik am Urteil vom Destrict Court und Federal Circuit - zudem mit Hinweis darauf, dass Richerin Du bei ihrem Urteil falsche juristische Standards angewendet hat und sie aufgrund dessen ein anderes" juristisches Verfahren" ( Grahamprinzip) zu berücksichtigen hat -
- Ablehnung der Klage von Amarin 👎
😇 MÖGE DIE GERECHTIGKEIT SIEGEN 😇
Am 21 Juni wird der SCOTUS dann sein Urteil bzgl. der Amarinklage bekanntgeben.
Hier noch einmal kurz zusammengefasst - die "Forderung" von Amarin an den SCOTUS :
Das Gericht sollte eine umfassende Überprüfung gewähren, um den Fehler in der Rechtssprechung des Bundesgerichtshofs zu korrigieren. Zumindest aber das Urteil aufzuheben und an den Bundesgerichtshof zurückzuweisen mit der Anweisung, nach dem Aspekt des "Grahamprinzips" juristisch vorzugehen bzw. zu verfahren.
Welche Entscheidung wird/könnte der SCOTUS fällen ?
Wie wird der Ausgang des Urteils Amarins Zukunft beeinflussen ?
Statistisch gesehen sind Amarins Gewinn-Chancen beim SCOTUS als sehr gering einzuschätzen.
MÖGLICHE SCOTUS-ENTSCHEIDUNGEN:
- Aufhebung des Urteils und Entscheidung für Amarin nach Anwendung des Grahamprinzips.👍
Der Supreme Court könnte rein theoretisch über die "Offensichtlichkeit" entscheiden. Ob er sich aber so intensiv mit dem Fall beschäftigen wird, um eine Entscheidung zu treffen, bezweifel ich stark, da u.a wissenschaftlich-technische Aspekte eine wichtige Rolle spielen und Aussagen von Experten von großer Bedeutung sein werden.
- Annahme der Amarin-Klage zur Verhandlung.👍
Eine Annahme des Falls durch den Supreme Court, um dann eine endgültige Entscheidung in einer späteren Verhandlung bzgl. der "Offensichtlichkeit" zu fällen - dieser juristische Schritt würde tendenziell bedeuten, dass große Zweifel am vorherigen Urteil bestünden.
- Aufhebung des Urteils und Rückverweisung an den Bundesgerichtshof👍
Ausgestattet mit deutlicher Kritik am Urteil vom Destrict Court und Federal Circuit - zudem mit Hinweis darauf, dass Richerin Du bei ihrem Urteil falsche juristische Standards angewendet hat und sie aufgrund dessen ein anderes" juristisches Verfahren" ( Grahamprinzip) zu berücksichtigen hat -
- Ablehnung der Klage von Amarin 👎
😇 MÖGE DIE GERECHTIGKEIT SIEGEN 😇
Antwort auf Beitrag Nr.: 68.306.081 von bernie55 am 26.05.21 12:44:57
MARJAC auf ihub: Übersetzt mit Translator
https://investorshub.advfn.com/boards/read_msg.aspx?message_…
Unsere Rule 60/Rule 24 Berufung wurde beim Federal Circuit eingereicht, Docket No.: 21-2024 für diejenigen, die zu Hause mitzählen.
Hier sind die wichtigsten Daten gemäß dem Federal Circuit's Life Cycle of an Appeal Guide:
9. August 2021: EPADI II Brief und Anhang sind fällig
20. September 2021: Hikma/Reddys Antwortbrief ist fällig
12. Oktober 2021: EPADI II Antwortschriftsatz fällig
19. Oktober 2021: Hard Copy Appendix wird beim Gericht eingereicht
Januar 2022: Mündliche Verhandlung angesetzt
Unten ist der Google Drive Link mit allen aktuellen Dokumenten. Da ich buchstäblich der Quarterback dieser Berufung bin, erhalte ich die Mitteilungen des Gerichts direkt. Sobald die Dokumente eingereicht werden, werde ich den Google Drive-Link so schnell wie möglich in diesem Board posten und unsere treuen Fans und Unterstützer auf dem Laufenden halten, sobald es soweit ist.
https://drive.google.com/drive/mobile/folders/16CAPwEghmsBDW…
Zitat von bernie55:Zitat von bernie55: Erste Reaktion von marjac auf i hub
Ich werde zurückkehren.
Eine Berufung beim Federal Circuit wird innerhalb von 30 Tagen erfolgen.
Die heutige Entscheidung ist gespickt mit Tatsachen- und Rechtsfehlern.
Ein Beispiel: "Der kritische Zeitpunkt für die Beurteilung der Rechtzeitigkeit eines Antrags auf Zulassung als Streithelfer ist der Zeitpunkt, an dem die vorgeschlagenen Streithelfer hätten erkennen müssen, dass ihre Interessen von den bestehenden Parteien nicht angemessen geschützt werden würden." Smith v. Los Angeles Unified School District, 830 F.3d 843, 854 (9th Cir. 2016). Entgegen der eindeutig fehlerhaften Schlussfolgerung von Richter Du ist dies in diesem Fall nicht geschehen, bis genügend Zeit nach dem Erhalt des Forderungsschreibens von eight durch Amarin verstrichen war, in der klar wurde, dass Amarin die Rule 60 nicht einreichen würde.
Darüber hinaus ist es ein klarer Fehler, die Rechtzeitigkeit unserer Einreichung unter Bezugnahme auf die Vorstadien des Rechtsstreits zu messen, die vor der Änderung der Umstände liegen, die unsere Entscheidung, dem Verfahren beizutreten, begründet haben. Id. bei 856. Hier hat Richter Du willkürlich verkündet, dass wir irgendwie während des Rechtsstreits hätten intervenieren sollen, obwohl wir in Wirklichkeit erst nach der Änderung der Umstände hätten intervenieren können, bestehend aus: (1) der Eintragung des Urteils am 30.3.2020; (2) der anschließenden Entdeckung des Irrtums und des Betrugs; und (3) der Entscheidung von Amarin, den Antrag nach Regel 60 nicht einzureichen, endgültig offensichtlich wurde.
Die Zeit, die seit Beginn des Rechtsstreits verstrichen ist, ist nicht ausschlaggebend, vielmehr musste das Gericht die damit zusammenhängenden Umstände betrachten, einschließlich des Zwecks, für den die Intervention beantragt wird. Id. Hier bestand der einzige Zweck der Intervention darin, die Rule 60 einzureichen, die vernünftigerweise nicht früher hätte eingereicht werden können, als wir sie eingereicht haben.
Dies ist nur eine Vorschau auf das, was dem Federal Circuit in der Berufung vorgelegt werden wird. Das heutige Ergebnis war enttäuschend, aber keineswegs das Ende des Weges.
Ich habe nicht vor, hier vor der Kammer ausführlich zu kommentieren, sondern unsere eingereichten Unterlagen werden für sich selbst sprechen.
https://investorshub.advfn.com/boards/read_msg.aspx?message_…
MARJAC hat neue Information im investorhub mitgeteilt. Er berichtet über einen anderen soliden rechtlichen aktuellen Präzedenzfall mit BETRUG. Klingt m.M.n. vielversprechend.
Unser Federal Circuit Appell hat gerade ein Geschenk erhalten. Hut ab vor Teammitglied Steve Lakey, der dieses Juwel gefunden hat.
Anfang dieses Monats bestätigte der Federal Circuit die Gewährung von Rule 60 Relief aufgrund von betrügerischen Expertenaussagen. Obwohl dieser Fall die Gewährung von Rule 60-Erleichterung bestätigte, können wir, während wir die Verweigerung der Rule 60-Erleichterung anstreben, diesen neuen Rule 60-Präzedenzfall dennoch mit großem Erfolg nutzen.
Ironischerweise wurde die Stellungnahme von Richter Dyk verfasst, dem sich Richter Hughes anschloss, die beide dem berüchtigten Rule 36 Panel in Amarins ursprünglicher Berufung angehörten.
Dies ist ein großartiges Omen, dass wir eine frische und faire Bewertung vom Federal Circuit erhalten können, da meine größte Sorge - die Zusammensetzung des Panels - vielleicht gar keine Sorge ist.
Dies ist ein positiver Beweis dafür, dass wir selbst dann, wenn wir die vermeintlich schlechteste Panel-Zusammensetzung erhalten, immer noch siegen können. Die in unserer Berufung vorgebrachten Punkte - Betrug, Irrtum, der nicht erzwungene breite, liberale Standard, der die Intervention regelt - sind ganz anders als die primären/sekundären Abwägungsfaktoren, die die Grundlage der Berufung von Amarin bilden, die derzeit vom Obersten Gerichtshof geprüft wird. Daher das Potenzial für eine günstigere Aufnahme.
Übersetzt mit Translator
https://investorshub.advfn.com/boards/read_msg.aspx?message_…
MARJAC auf ihub: Übersetzt mit Translator
https://investorshub.advfn.com/boards/read_msg.aspx?message_…
Unsere Rule 60/Rule 24 Berufung wurde beim Federal Circuit eingereicht, Docket No.: 21-2024 für diejenigen, die zu Hause mitzählen.
Hier sind die wichtigsten Daten gemäß dem Federal Circuit's Life Cycle of an Appeal Guide:
9. August 2021: EPADI II Brief und Anhang sind fällig
20. September 2021: Hikma/Reddys Antwortbrief ist fällig
12. Oktober 2021: EPADI II Antwortschriftsatz fällig
19. Oktober 2021: Hard Copy Appendix wird beim Gericht eingereicht
Januar 2022: Mündliche Verhandlung angesetzt
Unten ist der Google Drive Link mit allen aktuellen Dokumenten. Da ich buchstäblich der Quarterback dieser Berufung bin, erhalte ich die Mitteilungen des Gerichts direkt. Sobald die Dokumente eingereicht werden, werde ich den Google Drive-Link so schnell wie möglich in diesem Board posten und unsere treuen Fans und Unterstützer auf dem Laufenden halten, sobald es soweit ist.
https://drive.google.com/drive/mobile/folders/16CAPwEghmsBDW…
Antwort auf Beitrag Nr.: 68.447.858 von Magnetfeldfredy am 09.06.21 07:05:12
VAZKEPA® (icosapent ethyl): Revolutionising cardiovascular disease treatment
7th June 2021
Cardiovascular disease
© iStock/Tharakorn
Dr. Craig Granowitz, the Chief Medical Officer of pharmaceutical company Amarin Corporation, speaks to Health Europa about the never-ending pandemic, the number one cause of death in the European Union – cardiovascular disease – and how icosapent ethyl, Amarin’s novel treatment that is backed by robust clinical studies, can potentially revolutionise the future of cardiovascular therapy.
Cardiovascular disease is Europe’s leader in mortality, staggeringly equating to 3.9 million deaths on the continent each year, placing a substantial economic burden of €210 billion annually on the European Union; the requirement for innovations and advancements in cardiovascular treatment has never been more imperative. For the past 30 years, the traditional medications utilised to treat cardiovascular disease have been statins – a class of drugs that lower a patient’s levels of LDL cholesterol – which has been the principal focus of interventions in the disease. However, numerous primary and secondary prevention trials have demonstrated a residual risk beyond LDL cholesterol control of 65%-75%, a more comprehensive treatment is critical. It’s not that statins don’t serve a crucial purpose – they certainly do – they have saved millions of lives around the world and will continue to do so. The problem is that they are not the complete answer; they are an essential building block of cardiovascular treatment but not the complete solution.
In an arduous quest spanning nearly a decade, Amarin’s ground-breaking icosapent ethyl looks to fill the void of cardiovascular disease treatment, changing the landscape of future patient care. Icosapent ethyl has been meticulously examined by the REDUCE-IT study, which indicated that icosapent ethyl achieved a 25% relative risk reduction for cardiovascular events for patients with elevated triglyceride levels, these events being cardiovascular deaths, non-fatal heart attacks, non-fatal stroke, coronary revascularisation, and unstable angina. Additionally, the drug demonstrated relative risk reductions of 20% in cardiovascular deaths, 31% in heart attacks and 28% in strokes.. To discuss this innovative, life-saving medication, Health Europa sat down with industry expert and Amarin’s Chief Medical Officer, Dr Craig Granowitz to talk about all things cardiovascular disease.
Could you please give me an overview of yourself, your experience in the field of cardiovascular disease, and what the mission for Amarin is?
I have been with the company for about five and a half years, was here for the regulatory filings of the REDUCE-IT study, building all the science behind the epidemiology and the mechanisms of action we’ve been able to generate over the last several years. We’re very proud of the scientific advances that we’ve made in the field, developing 50-100 publications a year in support of the product and the category because I think the most important thing from the primary care market perspective is to highlight this issue of residual risk and that statins are a great part of the answer, but not the whole answer.
To do that, I think we needed to generate data, firstly in the US. Now we’ve been generating it in every European country that this is a significant public health crisis; it’s what we call the pandemic that is never-ending and hiding in plain sight. I don’t think there are enough pharma companies today investing back in public health and major diseases that impact millions of people. I think the industry has transitioned to speciality care products, injectable products, protein-based products, and oncology products. However, the vast majority of the disease still sits in primary care, and cardiovascular disease and diabetes is the nexus of all that. Going into what we’re doing for high-risk primary prevention is not typical of what pharma does today, so we’re really proud that we’re taking that on as a small company.
Across the World, the mortality rate for cardiovascular disease is enormous. Has the landscape of the condition improved over the last few years, or has there not been significant improvements year on year?
Well, there’s a difference between the number and the rate. The rate of cardiovascular disease, especially with many public health interventions like stopping smoking and antihypertensives, has meant that the rate of cardiovascular disease per age cohort has dropped for around 30 years but has now actually plateaued and is rising because of obesity, diabetes, and lifestyle. However, although the rate dropped, the population is rapidly ageing, so while the rate was dropping for each age cohort, the age cohorts that are rising are ones that have much higher rates of cardiovascular disease, so the overall number of cardiovascular disease for about two decades was offsetting, meaning the number of deaths and heart attacks was relatively stable. Now you’ve got both factors, both the demographic factor in terms of ageing and all the environmental factors working against us, so rates of cardiovascular disease are significantly on the rise in almost every country.
For example, in the 1970s in the UK, people ate a lot of meat, smoked a lot, didn’t manage their hypertension, and there were no statins, so the rates of heart disease were pretty high. Time passed, the air got a little cleaner, people became better educated, were exercising more, statins came on the market, hypertensives were used, and the healthcare providers did an excellent job. We saw the rates of cardiovascular disease were dropping. Furthermore, the UK population was ageing, so they offset each other, meaning the net deaths were either flat or slightly declining. However, today people eat much worse again, don’t exercise as much, have diabetes, and are older, so now all the things that were working are battling against you. Now you have a population that is still increasing in age, rising rates of diabetes, and the COVID-19 pandemic has exacerbated those trends even further because it preys on people with underlying health conditions, particularly cardiovascular disease, people stopped exercising and in turn gained weight.
For people with cardiovascular disease, how much has the COVID-19 pandemic impacted them?
I do not think we are going to know for quite some time. I think the early results in most countries show three main themes. The first is that COVID-19 preys on people with underlying cardiovascular disease, so it is accelerating morbidity and mortality. We will not be able to know how many people died of heart attacks and strokes either due to COVID-19 directly or cardiovascular disease. The next is that many people did not see their doctor or healthcare provider due to being in lockdown, fear of leaving the house, or healthcare providers not seeing them, so there is a lot of missing care for that period. The third is that many people during lockdown did not have healthy habits, the average person gained 10-20 pounds, alcohol consumption, smoking, and stress levels all rose. Studies of the UK’s excess morbidity and mortality have risen by 10% more deaths than the trendlines in the last year; a lot of that is probably caused due to cardiovascular disease.
© iStock/adamkaz
Do you think proper measures from healthcare providers were taken during this time for people with these underlying health conditions, and do you think lessons can be learned from this pandemic?
I think it was a reality of fear and prioritisation, not negligence. I think the issue and the focus on telehealth and remote medicine have some positive attributes. Still, especially for new medications, most healthcare providers are unwilling to make medication changes without physically seeing a patient. I can understand that because those are significant educational and potentially health implication impacts, I think they should rightfully be done face to face instead of over the internet or the phone. However, I believe that other solutions are being thought of using remote learning and remote education just like the rest of the world, I think some are helpful, and some are not so helpful.
Statins have been the traditionally used medication for cardiovascular disease for the last few decades. Could you explain how they work and potentially some of the shortfalls of the drug, why are they are not achieving the desired effect and should be used in tandem with another medication?
I think it’s a situation where people thought that because they had their statin that they had cardiovascular disease beaten. From looking at the patients in the REDUCE-IT study who received the placebo, more than one in four of them were well managed for all of their risk factors – including cholesterol. The average cholesterol was 74, the average in the UK is around 100 to 110, so they were all well managed for all of the well-known medical effects. Despite that, more than one in four patients over the period of 4.9 years had a heart attack, stroke, died of cardiovascular death, had a stent placed, or has unstable angina so symptomatic that they had to spend the night in a hospital. They are patients that are being well managed, not only with their statins but with their antihypertensives, diabetes medication, their antiplatelet medication if they needed it; these patients were on an average of 5-7 medications. Many of them had never had a cardiovascular event before. However, they had risk factors and diabetes, so the fact is that cardiovascular disease is still the number one or two cause of death in many countries, where each year it battles it out with cancer. In other western countries, cardiovascular disease is still well ahead of cancer.
Statins are not reducing the triglyceride levels that impact cardiovascular disease. Why has that not been studied further before?
Interestingly, in the 70s and 80s, everyone was focused on triglycerides because they are present in very high levels in the blood and cause damage to the blood vessels called plaque – kind of like rust on a pipe – most of the constituent is a lipid which is triglyceride. The problem is that triglycerides were too challenging to understand scientifically at the time, meaning the results that came out were confusing due to all of the feedback loops of triglycerides which are very difficult to study. Because of this, the world became captivated by the LDL receptor because it was easy to understand and was backed by some elegant science. Subsequently, the world switched to LDL and was a way that the pharmaceutical companies could develop highly effective therapies by inhibiting a single enzyme to a highly effective degree. Next, scientists believed that reducing LDL was good for cardiovascular disease, then raising another lipid called HDL is also good; the next ten years were spent fixated on these lipids. However, if you raise HDL, patients don’t have better outcomes, even though patients with low HDL have severe cardiovascular disease.
© iStock/rogerashford
Only our product – icosapent ethyl improves cardiovascular health but is independent of lowering triglycerides. In a sense, LDL is an excellent, simple marker to follow, but it doesn’t work in diabetes, it doesn’t work for HDL, it doesn’t work for triglycerides, with elevated levels of each of these resulting in worse patient outcomes. If you elevate those markers by themselves, you don’t improve human health. I think that is the main reason why triglycerides were put aside for 30 years, as it was simply too difficult for the science of the time to understand. It had a huge impact on the advancements of cardiovascular disease treatment; however, I do not want to take anything away from statins; they have saved millions of lives and still do.
Looking to the future of cardiovascular disease treatment, your team at Amarin have developed icosapent ethyl . Could you explain the benefits of the treatment, and should it be used alongside statins to provide a complete treatment for the disease?
This is really new science. I think what we have seen with fatty acids and omega 3’s, everyone thinks that they are the same, but they have remarkably different properties; that’s why individually, they’re called essential fatty acids. If they did the same thing, they wouldn’t be essential. Icosapent ethyl is a highly purified eicosapentaenoic acid (EPA), which is the only agent that has been demonstrated multiple times to lower cardiovascular events in appropriate patients. How does it work? Blood vessels have a lining called an endothelial cell – specialised cells that keep blood flowing when needed and stop blood flow when it shouldn’t. Under normal conditions, blood should flow without any vortices, and there should be a smooth laminar flow. The endothelial cell ensures that the blood vessel is optimally configured by interacting with the blood and underlying muscle and other tissue. But, if you get a cut in your arm, you want the endothelial cell to stop the bleeding, calling in clotting factors to do so. Because of this, the endothelial cell is exceptionally dynamic, possessing properties depending on what it is required to do, either anti-inflammatory or pro-inflammatory. What icosapent ethyl does is shield the endothelial cell; by entering the cell membrane it achieves numerous effects on the cell membrane itself but also triggers DNA and gene activation that allows the endothelial cell to be as healthy as it can be, responding normally to good signals and efficiently to bad signals, which is why the drug works so effectively. On the other hand, drugs like docosahexaenoic acid (DHA), which are other omega 3s, work in other tissues because they have different effects on the cell membrane and on genes. Icosapent ethyl is vital in keeping the blood vessels flowing, especially in people with diabetes, people who smoke, or have elevated cholesterol,. Essentially, icosapent ethyl is the right agent for the correct use in the right patient at the right time.
Icosapent ethyl has been rigorously analysed in the REDUCE-IT study. Could you explain that process, please? What were the results?
One of the reasons why many companies have left the cardiovascular space is that conducting these types of studies is extremely difficult and arduous. The study took seven years, was comprised of 8000 patients, totalling 40,000 patient-years analysed intensively, and cost $300 million, with possibly the most staggering part being that you didn’t know the answer until one day we all sat in a room and the data told us if the study was positive or negative. It’s an unbelievable task, an unbelievable achievement, which is a testament to all our staff, patients, investigators, and investors. That’s the level of evidence that the world, FDA, MHRA, EMA, and Canadian health authorities who have all approved icosapent ethyl, and only icosapent ethyl, expect and demand. We have been able to deliver that. We had unprecedented results, achieving a 25% relative risk reduction in cardiovascular events. To put that into perspective, it is a 5% absolute risk reduction which is unprecedented in this group of patients, which I believe is why we have been endorsed by 17.
different medical societies around the world, including the European Society of Cardiology (ESC), the European Atherosclerosis Society (EAS), both of whom recommended the use of the drug before it was even filed in Europe. We have been given approval from medical societies in both diabetes and cardiovascular disease in the US, as well as others in China, Egypt, and Argentina. In the US and Canada, we have been approved on an accelerated basis; we recently got first cycle approval in Europe with no clock stops and are one of the first drugs approved under the MHRA new system post-Brexit. The study results were so exceptional that the FDA brought in a secondary advisory group to analyse the study data and make a recommendation because the impact of the drug is so significant, they voted unanimously 16-0 in favour of approving icosapent ethyl.
Moving forward, what are the next steps before we see icosapent ethyl being implemented across Europe?
With regards to Europe, we are moving forward as fast as we can to seek reimbursement in ten major markets. Perhaps the most challenging thing in Europe is that processes differ in each country, with very few free markets with open pricing like the US. Usually, the adoption of any new medication in Europe tends to be a bit delayed because before the drug can be widely available, it needs to go through a rigorous economic and medical review process, which is what we’re doing right now in several European countries.
VAZKEPA® (icosapent ethyl): Revolutionising cardiovascular disease treatment
7th June 2021
Cardiovascular disease
© iStock/Tharakorn
Dr. Craig Granowitz, the Chief Medical Officer of pharmaceutical company Amarin Corporation, speaks to Health Europa about the never-ending pandemic, the number one cause of death in the European Union – cardiovascular disease – and how icosapent ethyl, Amarin’s novel treatment that is backed by robust clinical studies, can potentially revolutionise the future of cardiovascular therapy.
Cardiovascular disease is Europe’s leader in mortality, staggeringly equating to 3.9 million deaths on the continent each year, placing a substantial economic burden of €210 billion annually on the European Union; the requirement for innovations and advancements in cardiovascular treatment has never been more imperative. For the past 30 years, the traditional medications utilised to treat cardiovascular disease have been statins – a class of drugs that lower a patient’s levels of LDL cholesterol – which has been the principal focus of interventions in the disease. However, numerous primary and secondary prevention trials have demonstrated a residual risk beyond LDL cholesterol control of 65%-75%, a more comprehensive treatment is critical. It’s not that statins don’t serve a crucial purpose – they certainly do – they have saved millions of lives around the world and will continue to do so. The problem is that they are not the complete answer; they are an essential building block of cardiovascular treatment but not the complete solution.
In an arduous quest spanning nearly a decade, Amarin’s ground-breaking icosapent ethyl looks to fill the void of cardiovascular disease treatment, changing the landscape of future patient care. Icosapent ethyl has been meticulously examined by the REDUCE-IT study, which indicated that icosapent ethyl achieved a 25% relative risk reduction for cardiovascular events for patients with elevated triglyceride levels, these events being cardiovascular deaths, non-fatal heart attacks, non-fatal stroke, coronary revascularisation, and unstable angina. Additionally, the drug demonstrated relative risk reductions of 20% in cardiovascular deaths, 31% in heart attacks and 28% in strokes.. To discuss this innovative, life-saving medication, Health Europa sat down with industry expert and Amarin’s Chief Medical Officer, Dr Craig Granowitz to talk about all things cardiovascular disease.
Could you please give me an overview of yourself, your experience in the field of cardiovascular disease, and what the mission for Amarin is?
I have been with the company for about five and a half years, was here for the regulatory filings of the REDUCE-IT study, building all the science behind the epidemiology and the mechanisms of action we’ve been able to generate over the last several years. We’re very proud of the scientific advances that we’ve made in the field, developing 50-100 publications a year in support of the product and the category because I think the most important thing from the primary care market perspective is to highlight this issue of residual risk and that statins are a great part of the answer, but not the whole answer.
To do that, I think we needed to generate data, firstly in the US. Now we’ve been generating it in every European country that this is a significant public health crisis; it’s what we call the pandemic that is never-ending and hiding in plain sight. I don’t think there are enough pharma companies today investing back in public health and major diseases that impact millions of people. I think the industry has transitioned to speciality care products, injectable products, protein-based products, and oncology products. However, the vast majority of the disease still sits in primary care, and cardiovascular disease and diabetes is the nexus of all that. Going into what we’re doing for high-risk primary prevention is not typical of what pharma does today, so we’re really proud that we’re taking that on as a small company.
Across the World, the mortality rate for cardiovascular disease is enormous. Has the landscape of the condition improved over the last few years, or has there not been significant improvements year on year?
Well, there’s a difference between the number and the rate. The rate of cardiovascular disease, especially with many public health interventions like stopping smoking and antihypertensives, has meant that the rate of cardiovascular disease per age cohort has dropped for around 30 years but has now actually plateaued and is rising because of obesity, diabetes, and lifestyle. However, although the rate dropped, the population is rapidly ageing, so while the rate was dropping for each age cohort, the age cohorts that are rising are ones that have much higher rates of cardiovascular disease, so the overall number of cardiovascular disease for about two decades was offsetting, meaning the number of deaths and heart attacks was relatively stable. Now you’ve got both factors, both the demographic factor in terms of ageing and all the environmental factors working against us, so rates of cardiovascular disease are significantly on the rise in almost every country.
For example, in the 1970s in the UK, people ate a lot of meat, smoked a lot, didn’t manage their hypertension, and there were no statins, so the rates of heart disease were pretty high. Time passed, the air got a little cleaner, people became better educated, were exercising more, statins came on the market, hypertensives were used, and the healthcare providers did an excellent job. We saw the rates of cardiovascular disease were dropping. Furthermore, the UK population was ageing, so they offset each other, meaning the net deaths were either flat or slightly declining. However, today people eat much worse again, don’t exercise as much, have diabetes, and are older, so now all the things that were working are battling against you. Now you have a population that is still increasing in age, rising rates of diabetes, and the COVID-19 pandemic has exacerbated those trends even further because it preys on people with underlying health conditions, particularly cardiovascular disease, people stopped exercising and in turn gained weight.
For people with cardiovascular disease, how much has the COVID-19 pandemic impacted them?
I do not think we are going to know for quite some time. I think the early results in most countries show three main themes. The first is that COVID-19 preys on people with underlying cardiovascular disease, so it is accelerating morbidity and mortality. We will not be able to know how many people died of heart attacks and strokes either due to COVID-19 directly or cardiovascular disease. The next is that many people did not see their doctor or healthcare provider due to being in lockdown, fear of leaving the house, or healthcare providers not seeing them, so there is a lot of missing care for that period. The third is that many people during lockdown did not have healthy habits, the average person gained 10-20 pounds, alcohol consumption, smoking, and stress levels all rose. Studies of the UK’s excess morbidity and mortality have risen by 10% more deaths than the trendlines in the last year; a lot of that is probably caused due to cardiovascular disease.
© iStock/adamkaz
Do you think proper measures from healthcare providers were taken during this time for people with these underlying health conditions, and do you think lessons can be learned from this pandemic?
I think it was a reality of fear and prioritisation, not negligence. I think the issue and the focus on telehealth and remote medicine have some positive attributes. Still, especially for new medications, most healthcare providers are unwilling to make medication changes without physically seeing a patient. I can understand that because those are significant educational and potentially health implication impacts, I think they should rightfully be done face to face instead of over the internet or the phone. However, I believe that other solutions are being thought of using remote learning and remote education just like the rest of the world, I think some are helpful, and some are not so helpful.
Statins have been the traditionally used medication for cardiovascular disease for the last few decades. Could you explain how they work and potentially some of the shortfalls of the drug, why are they are not achieving the desired effect and should be used in tandem with another medication?
I think it’s a situation where people thought that because they had their statin that they had cardiovascular disease beaten. From looking at the patients in the REDUCE-IT study who received the placebo, more than one in four of them were well managed for all of their risk factors – including cholesterol. The average cholesterol was 74, the average in the UK is around 100 to 110, so they were all well managed for all of the well-known medical effects. Despite that, more than one in four patients over the period of 4.9 years had a heart attack, stroke, died of cardiovascular death, had a stent placed, or has unstable angina so symptomatic that they had to spend the night in a hospital. They are patients that are being well managed, not only with their statins but with their antihypertensives, diabetes medication, their antiplatelet medication if they needed it; these patients were on an average of 5-7 medications. Many of them had never had a cardiovascular event before. However, they had risk factors and diabetes, so the fact is that cardiovascular disease is still the number one or two cause of death in many countries, where each year it battles it out with cancer. In other western countries, cardiovascular disease is still well ahead of cancer.
Statins are not reducing the triglyceride levels that impact cardiovascular disease. Why has that not been studied further before?
Interestingly, in the 70s and 80s, everyone was focused on triglycerides because they are present in very high levels in the blood and cause damage to the blood vessels called plaque – kind of like rust on a pipe – most of the constituent is a lipid which is triglyceride. The problem is that triglycerides were too challenging to understand scientifically at the time, meaning the results that came out were confusing due to all of the feedback loops of triglycerides which are very difficult to study. Because of this, the world became captivated by the LDL receptor because it was easy to understand and was backed by some elegant science. Subsequently, the world switched to LDL and was a way that the pharmaceutical companies could develop highly effective therapies by inhibiting a single enzyme to a highly effective degree. Next, scientists believed that reducing LDL was good for cardiovascular disease, then raising another lipid called HDL is also good; the next ten years were spent fixated on these lipids. However, if you raise HDL, patients don’t have better outcomes, even though patients with low HDL have severe cardiovascular disease.
© iStock/rogerashford
Only our product – icosapent ethyl improves cardiovascular health but is independent of lowering triglycerides. In a sense, LDL is an excellent, simple marker to follow, but it doesn’t work in diabetes, it doesn’t work for HDL, it doesn’t work for triglycerides, with elevated levels of each of these resulting in worse patient outcomes. If you elevate those markers by themselves, you don’t improve human health. I think that is the main reason why triglycerides were put aside for 30 years, as it was simply too difficult for the science of the time to understand. It had a huge impact on the advancements of cardiovascular disease treatment; however, I do not want to take anything away from statins; they have saved millions of lives and still do.
Looking to the future of cardiovascular disease treatment, your team at Amarin have developed icosapent ethyl . Could you explain the benefits of the treatment, and should it be used alongside statins to provide a complete treatment for the disease?
This is really new science. I think what we have seen with fatty acids and omega 3’s, everyone thinks that they are the same, but they have remarkably different properties; that’s why individually, they’re called essential fatty acids. If they did the same thing, they wouldn’t be essential. Icosapent ethyl is a highly purified eicosapentaenoic acid (EPA), which is the only agent that has been demonstrated multiple times to lower cardiovascular events in appropriate patients. How does it work? Blood vessels have a lining called an endothelial cell – specialised cells that keep blood flowing when needed and stop blood flow when it shouldn’t. Under normal conditions, blood should flow without any vortices, and there should be a smooth laminar flow. The endothelial cell ensures that the blood vessel is optimally configured by interacting with the blood and underlying muscle and other tissue. But, if you get a cut in your arm, you want the endothelial cell to stop the bleeding, calling in clotting factors to do so. Because of this, the endothelial cell is exceptionally dynamic, possessing properties depending on what it is required to do, either anti-inflammatory or pro-inflammatory. What icosapent ethyl does is shield the endothelial cell; by entering the cell membrane it achieves numerous effects on the cell membrane itself but also triggers DNA and gene activation that allows the endothelial cell to be as healthy as it can be, responding normally to good signals and efficiently to bad signals, which is why the drug works so effectively. On the other hand, drugs like docosahexaenoic acid (DHA), which are other omega 3s, work in other tissues because they have different effects on the cell membrane and on genes. Icosapent ethyl is vital in keeping the blood vessels flowing, especially in people with diabetes, people who smoke, or have elevated cholesterol,. Essentially, icosapent ethyl is the right agent for the correct use in the right patient at the right time.
Icosapent ethyl has been rigorously analysed in the REDUCE-IT study. Could you explain that process, please? What were the results?
One of the reasons why many companies have left the cardiovascular space is that conducting these types of studies is extremely difficult and arduous. The study took seven years, was comprised of 8000 patients, totalling 40,000 patient-years analysed intensively, and cost $300 million, with possibly the most staggering part being that you didn’t know the answer until one day we all sat in a room and the data told us if the study was positive or negative. It’s an unbelievable task, an unbelievable achievement, which is a testament to all our staff, patients, investigators, and investors. That’s the level of evidence that the world, FDA, MHRA, EMA, and Canadian health authorities who have all approved icosapent ethyl, and only icosapent ethyl, expect and demand. We have been able to deliver that. We had unprecedented results, achieving a 25% relative risk reduction in cardiovascular events. To put that into perspective, it is a 5% absolute risk reduction which is unprecedented in this group of patients, which I believe is why we have been endorsed by 17.
different medical societies around the world, including the European Society of Cardiology (ESC), the European Atherosclerosis Society (EAS), both of whom recommended the use of the drug before it was even filed in Europe. We have been given approval from medical societies in both diabetes and cardiovascular disease in the US, as well as others in China, Egypt, and Argentina. In the US and Canada, we have been approved on an accelerated basis; we recently got first cycle approval in Europe with no clock stops and are one of the first drugs approved under the MHRA new system post-Brexit. The study results were so exceptional that the FDA brought in a secondary advisory group to analyse the study data and make a recommendation because the impact of the drug is so significant, they voted unanimously 16-0 in favour of approving icosapent ethyl.
Moving forward, what are the next steps before we see icosapent ethyl being implemented across Europe?
With regards to Europe, we are moving forward as fast as we can to seek reimbursement in ten major markets. Perhaps the most challenging thing in Europe is that processes differ in each country, with very few free markets with open pricing like the US. Usually, the adoption of any new medication in Europe tends to be a bit delayed because before the drug can be widely available, it needs to go through a rigorous economic and medical review process, which is what we’re doing right now in several European countries.
Antwort auf Beitrag Nr.: 68.433.404 von bernie55 am 07.06.21 22:03:17
Super Bernie!
Scripts stabil gut, bei dieser "Runrate" würde Amarin alleine in den USA ca. 700 Millionen US $ Umsatz machen, alleine für diesen Umsatz müste die Marktkapitalisierung bei 3,5-4 Milliarden US $ sein, wir sind bei der Hälfte.....
Dazu Europa und ROW.... KZ US Dollar 20!
Super Bernie!
Scripts stabil gut, bei dieser "Runrate" würde Amarin alleine in den USA ca. 700 Millionen US $ Umsatz machen, alleine für diesen Umsatz müste die Marktkapitalisierung bei 3,5-4 Milliarden US $ sein, wir sind bei der Hälfte.....
Dazu Europa und ROW.... KZ US Dollar 20!

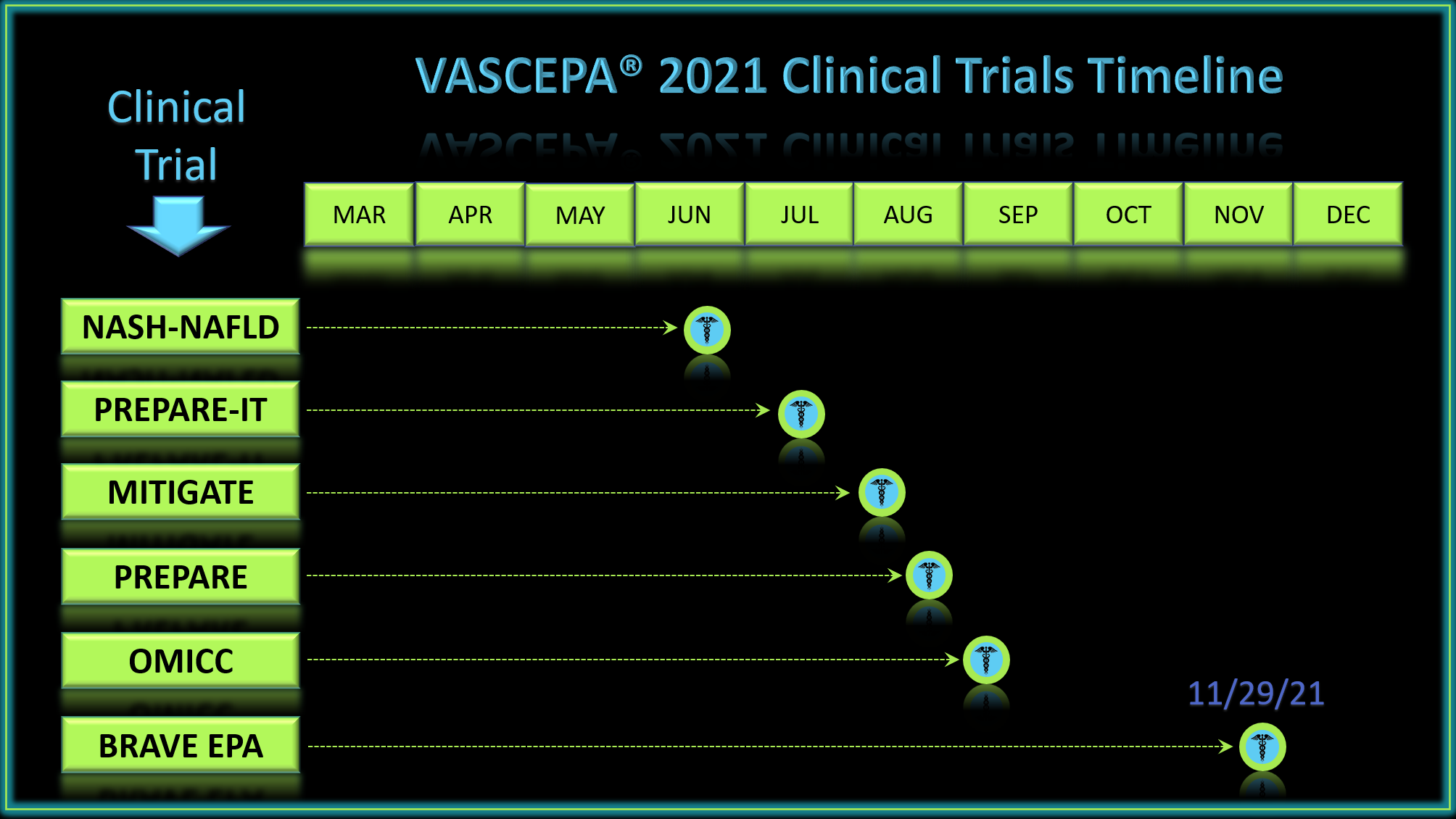
Möglicher Zeitplan bevorstehender klinischer Ergebnisse mit Vascepa in 2021 ( von CaptBeer auf stocktwits)
Amarin - The Science Of Lipid Therapy



















