



CytomX - ein bahnbrechender Ansatz in der Tumortherapie (Seite 109)
eröffnet am 01.07.16 16:03:16 von
neuester Beitrag 01.05.24 17:27:40 von
neuester Beitrag 01.05.24 17:27:40 von
Beiträge: 1.462
ID: 1.234.534
ID: 1.234.534
Aufrufe heute: 18
Gesamt: 164.124
Gesamt: 164.124
Aktive User: 0
ISIN: US23284F1057 · WKN: A14158 · Symbol: 6C1
4,1240
EUR
-1,01 %
-0,0420 EUR
Letzter Kurs 03.05.24 Tradegate
Neuigkeiten
02.05.24 · wO Chartvergleich |
02.05.24 · Sharedeals |
01.05.24 · globenewswire |
08.04.24 · globenewswire |
Werte aus der Branche Biotechnologie
| Wertpapier | Kurs | Perf. % |
|---|---|---|
| 38,27 | +28,16 | |
| 8,0780 | +27,90 | |
| 10,155 | +21,04 | |
| 8,1400 | +20,41 | |
| 3,6100 | +17,51 |
| Wertpapier | Kurs | Perf. % |
|---|---|---|
| 0,6700 | -26,58 | |
| 2,1300 | -34,41 | |
| 3,1600 | -38,64 | |
| 1,7000 | -49,40 | |
| 125,00 | -95,83 |
Beitrag zu dieser Diskussion schreiben
Antwort auf Beitrag Nr.: 55.554.792 von fme_wo am 18.08.17 18:10:21Das dürfte auch der Grund für den heutigen abverkauf sein. Der gute Herr ist nun bei FPRX .
Antwort auf Beitrag Nr.: 55.556.016 von Ville7 am 18.08.17 20:42:01"die Vielfache Menge im Körper zirkulieren.." -> natürlich die vielfache Menge im Vgl. zu einem herkömmlichen PD-L1 AK.
Antwort auf Beitrag Nr.: 55.483.191 von Ville7 am 08.08.17 20:13:45Cytomx geht bei Proclaim-CX-072 übrigens nach dem klassischen 3 plus 3 Schema vor:
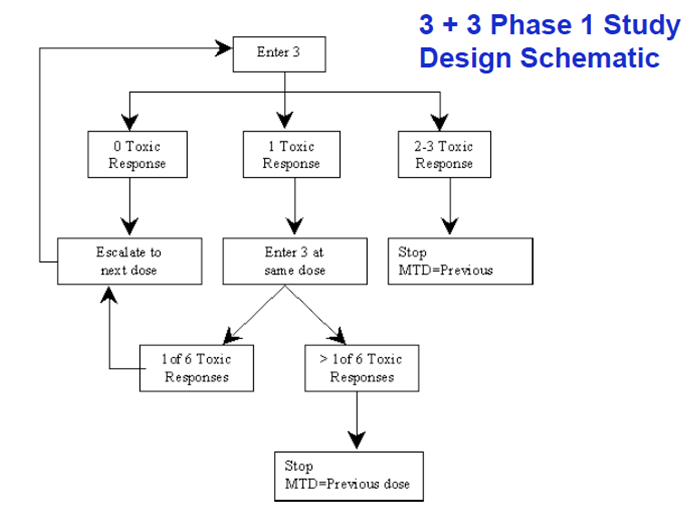
Ich persönlich stelle mir die Frage, was sie machen, wenn 30mg/kg noch keine Dosisbegrenzung darstellt. Noch höher dosieren oder bei 30mg/kg aufhören? Schließlich sollte bereits bei 10mg/kg die Vielfache Menge im Körper zirkulieren...
Ich persönlich stelle mir die Frage, was sie machen, wenn 30mg/kg noch keine Dosisbegrenzung darstellt. Noch höher dosieren oder bei 30mg/kg aufhören? Schließlich sollte bereits bei 10mg/kg die Vielfache Menge im Körper zirkulieren...
Zitat von Ville7: Wir sollten nun an der orangenen Linie sein:
@Joschka, es ist doch üblich die Anzahl der Patienten in den höheren Dosis-Gruppen zu erhöhen, oder? Wenn ich linear hochrechne wären wir mit multipler Dosierung frühestens sogar im Januar 2018 fertig bis zur höchsten Dosis in allen Gruppen - ohne expansion cohort Part D. Erste Daten zu ASCO 2018 sollten somit m.E. drin sein.

Eine Führungskraft hat CytomX verlassen: https://globenewswire.com/news-release/2017/08/17/1088296/0/…
Da kann man sich fragen, warum in dieser doch eigentlich spannenden Phase. Oder ist aus Forschungssicht der spannendste Teil bereits durch?
Da kann man sich fragen, warum in dieser doch eigentlich spannenden Phase. Oder ist aus Forschungssicht der spannendste Teil bereits durch?
Antwort auf Beitrag Nr.: 55.542.453 von biopadawan am 17.08.17 11:36:57
Yep, zum ersten Mal von Debanjan Ray präsentiert. Es war nichts unterschwellig Neues zu erfahren...
Zitat von biopadawan: Auf der Unternehmenshomepage wurden der Audio Webcast sowie die Unternehmenspräsentation vom 16.08.2017 online gestellt.
http://ir.cytomx.com/phoenix.zhtml?c=254195&p=irol-irhome
Yep, zum ersten Mal von Debanjan Ray präsentiert. Es war nichts unterschwellig Neues zu erfahren...
Trading Spotlight
Auf der Unternehmenshomepage wurden der Audio Webcast sowie die Unternehmenspräsentation vom 16.08.2017 online gestellt.
http://ir.cytomx.com/phoenix.zhtml?c=254195&p=irol-irhome
http://ir.cytomx.com/phoenix.zhtml?c=254195&p=irol-irhome
Antwort auf Beitrag Nr.: 55.541.493 von Ville7 am 17.08.17 09:36:51Korrektur: "trotz des Misserfolgs in PFS und trotz der erhöhten Nebenwirkungen" !
Das Scheitern von BMS in 1st line RCC sehe ich persönlich mit einem lachenden Auge, da es meine EXEL (Cabozantinib) begünstigt. Die haben dann auch gleich gestern ihr 1st line filing auf Basis der CaboSun Daten Richtung FDA auf den Weg gebracht. So weit off topic... zurück zu der BMS Studie: ich denke, dass BMS trotz des Misserfolgs und trotz der erhöhten Nebenwirkungen in PFS auf Basis von OS Daten einen Zulassungsantrag in 1st line RCC stellen wird.
Perfekt wäre es, sollte die CTMX Technologie funktionieren, wenn man nicht nur Biologics maskieren könnte, sondern auch small molecules. Und noch perfekter, wenn dies sogar bei oraler Verabreichung gehen würde, sodass sogar z.B. orale TKIs maskiert werden könnten. Aber ich denke der Verdauungsapparat würde da sofort die Maskierung "verdauen" bzw. zerstören....
Perfekt wäre es, sollte die CTMX Technologie funktionieren, wenn man nicht nur Biologics maskieren könnte, sondern auch small molecules. Und noch perfekter, wenn dies sogar bei oraler Verabreichung gehen würde, sodass sogar z.B. orale TKIs maskiert werden könnten. Aber ich denke der Verdauungsapparat würde da sofort die Maskierung "verdauen" bzw. zerstören....
Antwort auf Beitrag Nr.: 55.531.719 von Joschka Schröder am 16.08.17 00:19:48Wobei ich einen Endpunkt "progressionsfreies Überleben" bei einer Immuntherapie(-Kombi) immer noch als falsch gewählt ansehe.
Zu meinen Medarex-Investor-Zeiten (mir kommt immer noch die Galle hoch, dass ich damals so billig von Pien und BMS enteignet wurde, denn sonst könnte ich schon finanziell unabhängig sein) war bereits klar ersichtlich, dass ipilimumab keine statistisch signifikanten PFS Vorteile erzeugen konnte, aber das Gesamtüberleben sehr sehr positiv beeinflusst wurde. Etwas, was die Zulassungsbehörden damals noch nicht wirklich verstanden haben...
Ich könnte mir vorstellen, dass ähnliche Effekte bei einer Kombi wirken. anti-PD(L1) scheint ja mehr PFS Vorteile zu bedingen als anti-CTLA-4 (wo diese Vorteile kaum zu beobachten sind).
Für eine Kombi, bei der beide Kombipartner niedriger dosiert werden müssen, ist m.E. das Gesamtüberleben der richtigere Endpunkt.
Und klar, die Nebenwirkungen sind DER limitierende Faktor! Das ist das Thema um das es bei CTMX geht. Falls die CTMX probodies funktionieren, sollten diese kombiniert sowohl PFS als auch gigantische OS Vorteile bedingen.
Spannend wird es in den nächsten 12 Monaten allemal. Nichts oder Alles. Und wenn Alles, dann ist das sicherlich ein großes Vielfaches von Jetzt. Zudem könnte es eine Achterbahnfahrt werden (CX-2009 scheitert, CX-072 trotzdem Erfolg), also anschnallen.
Meine Paranoia werde ich bis dahin nicht ablegen und weiter nach allen Haaren in der Suppe suchen.
Zu meinen Medarex-Investor-Zeiten (mir kommt immer noch die Galle hoch, dass ich damals so billig von Pien und BMS enteignet wurde, denn sonst könnte ich schon finanziell unabhängig sein) war bereits klar ersichtlich, dass ipilimumab keine statistisch signifikanten PFS Vorteile erzeugen konnte, aber das Gesamtüberleben sehr sehr positiv beeinflusst wurde. Etwas, was die Zulassungsbehörden damals noch nicht wirklich verstanden haben...
Ich könnte mir vorstellen, dass ähnliche Effekte bei einer Kombi wirken. anti-PD(L1) scheint ja mehr PFS Vorteile zu bedingen als anti-CTLA-4 (wo diese Vorteile kaum zu beobachten sind).
Für eine Kombi, bei der beide Kombipartner niedriger dosiert werden müssen, ist m.E. das Gesamtüberleben der richtigere Endpunkt.
Und klar, die Nebenwirkungen sind DER limitierende Faktor! Das ist das Thema um das es bei CTMX geht. Falls die CTMX probodies funktionieren, sollten diese kombiniert sowohl PFS als auch gigantische OS Vorteile bedingen.
Spannend wird es in den nächsten 12 Monaten allemal. Nichts oder Alles. Und wenn Alles, dann ist das sicherlich ein großes Vielfaches von Jetzt. Zudem könnte es eine Achterbahnfahrt werden (CX-2009 scheitert, CX-072 trotzdem Erfolg), also anschnallen.
Meine Paranoia werde ich bis dahin nicht ablegen und weiter nach allen Haaren in der Suppe suchen.
Enttäuschende Daten aus der CheckMate-214-Studie! Eine weitere Dosiserhöhung des Checkpointinhibitors Opdivo oder des anti-CTLA-4-Antikörpers Yervoy wäre wegen der starken Nebenwirkungen der Präparate (s. Ende der Meldung) nicht möglich. Hier könnte und sollte CytomX´s Probody-Technologie Abhilfe schaffen. Als Alternative für die besagte Opdivo/Yervoy-Kombi böte sich eine Kombinationstherapie z.B. aus CX-072 (CytomX) und dem anti-CTLA-4-Probody (CytomX/BMY) an. Hier sollte man - zumindest in der Therorie - deutlich höher dosieren können, ohne dass unakzeptable Nebenwirkungen auftreten.
Tuesday, August 15, 2017 4:30 pm EDT
PRINCETON, N.J.--(BUSINESS WIRE)--Bristol-Myers Squibb Company (NYSE: BMY) announced topline results today from the CheckMate -214 trial investigating Opdivo (nivolumab) in combination with Yervoy (ipilimumab) versus sunitinib in intermediate and poor-risk patients previously untreated advanced or metastatic renal cell carcinoma. The combination met the co-primary endpoint of objective response rate (ORR) and achieved a 41.6% ORR versus 26.5% for sunitinib. Median duration of response was not reached for the combination of Opdivo and Yervoy and was 18.17 months for sunitinib. While there was an improvement in progression-free survival (PFS) (HR=0.82, [95% CI 0.64 – 1.05]; stratified 2-sided p=0.03), it did not reach statistical significance. The median PFS was 11.56 months (95% CI 8.71 – 15.51) for the Opdivo and Yervoy combination versus 8.38 months (95% CI 7.03-10.81) for sunitinib, The study will continue as planned to allow the third co-primary endpoint of overall survival to mature. The tolerability profile observed in CheckMate-214 was consistent with that observed in previously reported studies of this dosing schedule.
“We are encouraged by the totality of the CheckMate-214 data. The overall response rate and durability of response favored the combination of Opdivo and Yervoy, and the trend for PFS supports the potential of the combination in intermediate and poor-risk advanced renal cell carcinoma, the most common type of kidney cancer. This is an important study in first-line renal cancer as these patients need new options,” said Vicki Goodman, M.D., development lead, Melanoma and Genitourinary Cancers, Bristol-Myers Squibb. “We look forward to presenting the full results from this study at an upcoming medical meeting.”
“Opdivo is now well established as standard of care in the treatment of second-line renal cell carcinoma,” said Goodman. “The company plans to share these important first-line data with regulatory authorities and we look forward to reporting overall survival when these data mature.”
About CheckMate -214
CheckMate -214 is a phase 3, randomized, open-label study evaluating the combination of Opdivo plus Yervoy versus sunitinib in patients with previously untreated advanced or metastatic renal cell carcinoma. Patients in the combination group received Opdivo 3 mg/kg plus Yervoy 1 mg/kg every 3 weeks for 4 doses followed by Opdivo 3 mg/kg every 2 weeks. Patients in the comparator group received sunitinib 50 mg once daily for 4 weeks, followed by 2 weeks off before continuation of treatment. Patients were treated until progression or unacceptable toxic effects. The primary endpoints of the trial are progression-free survival, overall survival and objective response rate in an intermediate to poor-risk patient population (approximately 75 percent of patients). The majority of alpha was allocated to overall survival. Safety is a secondary endpoint.
...
IMPORTANT SAFETY INFORMATION
WARNING: IMMUNE-MEDIATED ADVERSE REACTIONS
YERVOY can result in severe and fatal immune-mediated adverse reactions. These immune-mediated reactions may involve any organ system; however, the most common severe immune-mediated adverse reactions are enterocolitis, hepatitis, dermatitis (including toxic epidermal necrolysis), neuropathy, and endocrinopathy. The majority of these immune-mediated reactions initially manifested during treatment; however, a minority occurred weeks to months after discontinuation of YERVOY.
Assess patients for signs and symptoms of enterocolitis, dermatitis, neuropathy, and endocrinopathy and evaluate clinical chemistries including liver function tests (LFTs), adrenocorticotropic hormone (ACTH) level, and thyroid function tests at baseline and before each dose.
Permanently discontinue YERVOY and initiate systemic high-dose corticosteroid therapy for severe immune-mediated reactions.
Immune-Mediated Pneumonitis
OPDIVO can cause immune-mediated pneumonitis. Fatal cases have been reported. Monitor patients for signs with radiographic imaging and for symptoms of pneumonitis. Administer corticosteroids for Grade 2 or more severe pneumonitis. Permanently discontinue for Grade 3 or 4 and withhold until resolution for Grade 2. In patients receiving OPDIVO monotherapy, fatal cases of immune-mediated pneumonitis have occurred. Immune-mediated pneumonitis occurred in 3.1% (61/1994) of patients. In patients receiving OPDIVO with YERVOY, immune-mediated pneumonitis occurred in 6% (25/407) of patients.
In Checkmate 205 and 039, pneumonitis, including interstitial lung disease, occurred in 6.0% (16/266) of patients receiving OPDIVO. Immune-mediated pneumonitis occurred in 4.9% (13/266) of patients receiving OPDIVO: Grade 3 (n=1) and Grade 2 (n=12).
Immune-Mediated Colitis
OPDIVO can cause immune-mediated colitis. Monitor patients for signs and symptoms of colitis. Administer corticosteroids for Grade 2 (of more than 5 days duration), 3, or 4 colitis. Withhold OPDIVO monotherapy for Grade 2 or 3 and permanently discontinue for Grade 4 or recurrent colitis upon re-initiation of OPDIVO. When administered with YERVOY, withhold OPDIVO and YERVOY for Grade 2 and permanently discontinue for Grade 3 or 4 or recurrent colitis. In patients receiving OPDIVO monotherapy, immune-mediated colitis occurred in 2.9% (58/1994) of patients. In patients receiving OPDIVO with YERVOY, immune-mediated colitis occurred in 26% (107/407) of patients including three fatal cases.
In a separate Phase 3 study of YERVOY 3 mg/kg, severe, life-threatening, or fatal (diarrhea of ≥7 stools above baseline, fever, ileus, peritoneal signs; Grade 3-5) immune-mediated enterocolitis occurred in 34 (7%) patients. Across all YERVOY-treated patients in that study (n=511), 5 (1%) developed intestinal perforation, 4 (0.8%) died as a result of complications, and 26 (5%) were hospitalized for severe enterocolitis.
Immune-Mediated Hepatitis
OPDIVO can cause immune-mediated hepatitis. Monitor patients for abnormal liver tests prior to and periodically during treatment. Administer corticosteroids for Grade 2 or greater transaminase elevations. Withhold for Grade 2 and permanently discontinue for Grade 3 or 4 immune-mediated hepatitis. In patients receiving OPDIVO monotherapy, immune-mediated hepatitis occurred in 1.8% (35/1994) of patients. In patients receiving OPDIVO with YERVOY, immune-mediated hepatitis occurred in 13% (51/407) of patients.
In a separate Phase 3 study of YERVOY 3 mg/kg, severe, life-threatening, or fatal hepatotoxicity (AST or ALT elevations >5x the ULN or total bilirubin elevations >3x the ULN; Grade 3-5) occurred in 8 (2%) patients, with fatal hepatic failure in 0.2% and hospitalization in 0.4%.
Immune-Mediated Neuropathies
In a separate Phase 3 study of YERVOY 3 mg/kg, 1 case of fatal Guillain-Barré syndrome and 1 case of severe (Grade 3) peripheral motor neuropathy were reported.
Immune-Mediated Endocrinopathies
OPDIVO can cause immune-mediated hypophysitis, immune-mediated adrenal insufficiency, autoimmune thyroid disorders, and Type 1 diabetes mellitus. Monitor patients for signs and symptoms of hypophysitis, signs and symptoms of adrenal insufficiency, thyroid function prior to and periodically during treatment, and hyperglycemia. Administer hormone replacement as clinically indicated and corticosteroids for Grade 2 or greater hypophysitis. Withhold for Grade 2 or 3 and permanently discontinue for Grade 4 hypophysitis. Administer corticosteroids for Grade 3 or 4 adrenal insufficiency. Withhold for Grade 2 and permanently discontinue for Grade 3 or 4 adrenal insufficiency. Administer hormone-replacement therapy for hypothyroidism. Initiate medical management for control of hyperthyroidism. Withhold OPDIVO for Grade 3 and permanently discontinue for Grade 4 hyperglycemia.
In patients receiving OPDIVO monotherapy, hypophysitis occurred in 0.6% (12/1994) of patients. In patients receiving OPDIVO with YERVOY, hypophysitis occurred in 9% (36/407) of patients. In patients receiving OPDIVO monotherapy, adrenal insufficiency occurred in 1% (20/1994) of patients. In patients receiving OPDIVO with YERVOY, adrenal insufficiency occurred in 5% (21/407) of patients. In patients receiving OPDIVO monotherapy, hypothyroidism or thyroiditis resulting in hypothyroidism occurred in 9% (171/1994) of patients. Hyperthyroidism occurred in 2.7% (54/1994) of patients receiving OPDIVO monotherapy. In patients receiving OPDIVO with YERVOY, hypothyroidism or thyroiditis resulting in hypothyroidism occurred in 22% (89/407) of patients. Hyperthyroidism occurred in 8% (34/407) of patients receiving OPDIVO with YERVOY. In patients receiving OPDIVO monotherapy, diabetes occurred in 0.9% (17/1994) of patients. In patients receiving OPDIVO with YERVOY, diabetes occurred in 1.5% (6/407) of patients.
In a separate Phase 3 study of YERVOY 3 mg/kg, severe to life-threatening immune-mediated endocrinopathies (requiring hospitalization, urgent medical intervention, or interfering with activities of daily living; Grade 3-4) occurred in 9 (1.8%) patients. All 9 patients had hypopituitarism, and some had additional concomitant endocrinopathies such as adrenal insufficiency, hypogonadism, and hypothyroidism. 6 of the 9 patients were hospitalized for severe endocrinopathies.
Immune-Mediated Nephritis and Renal Dysfunction
OPDIVO can cause immune-mediated nephritis. Monitor patients for elevated serum creatinine prior to and periodically during treatment. Administer corticosteroids for Grades 2-4 increased serum creatinine. Withhold OPDIVO for Grade 2 or 3 and permanently discontinue for Grade 4 increased serum creatinine. In patients receiving OPDIVO monotherapy, immune-mediated nephritis and renal dysfunction occurred in 1.2% (23/1994) of patients. In patients receiving OPDIVO with YERVOY, immune-mediated nephritis and renal dysfunction occurred in 2.2% (9/407) of patients.
Immune-Mediated Skin Adverse Reactions and Dermatitis
OPDIVO can cause immune-mediated rash, including Stevens-Johnson syndrome (SJS) and toxic epidermal necrolysis (TEN), some cases with fatal outcome. Administer corticosteroids for Grade 3 or 4 rash. Withhold for Grade 3 and permanently discontinue for Grade 4 rash. For symptoms or signs of SJS or TEN, withhold OPDIVO and refer the patient for specialized care for assessment and treatment; if confirmed, permanently discontinue. In patients receiving OPDIVO monotherapy, immune-mediated rash occurred in 9% (171/1994) of patients. In patients receiving OPDIVO with YERVOY, immune-mediated rash occurred in 22.6% (92/407) of patients.
In a separate Phase 3 study of YERVOY 3 mg/kg, severe, life-threatening, or fatal immune-mediated dermatitis (eg, Stevens-Johnson syndrome, toxic epidermal necrolysis, or rash complicated by full thickness dermal ulceration, or necrotic, bullous, or hemorrhagic manifestations; Grade 3-5) occurred in 13 (2.5%) patients. 1 (0.2%) patient died as a result of toxic epidermal necrolysis. 1 additional patient required hospitalization for severe dermatitis.
Immune-Mediated Encephalitis
OPDIVO can cause immune-mediated encephalitis. Evaluation of patients with neurologic symptoms may include, but not be limited to, consultation with a neurologist, brain MRI, and lumbar puncture. Withhold OPDIVO in patients with new-onset moderate to severe neurologic signs or symptoms and evaluate to rule out other causes. If other etiologies are ruled out, administer corticosteroids and permanently discontinue OPDIVO for immune-mediated encephalitis. In patients receiving OPDIVO monotherapy, encephalitis occurred in 0.2% (3/1994) of patients. Fatal limbic encephalitis occurred in one patient after 7.2 months of exposure despite discontinuation of OPDIVO and administration of corticosteroids. Encephalitis occurred in one patient receiving OPDIVO with YERVOY (0.2%) after 1.7 months of exposure.
Other Immune-Mediated Adverse Reactions
Based on the severity of adverse reaction, permanently discontinue or withhold treatment, administer high-dose corticosteroids, and, if appropriate, initiate hormone-replacement therapy. Across clinical trials of OPDIVO the following clinically significant immune-mediated adverse reactions occurred in <1.0% of patients receiving OPDIVO: uveitis, iritis, pancreatitis, facial and abducens nerve paresis, demyelination, polymyalgia rheumatica, autoimmune neuropathy, Guillain-Barré syndrome, hypopituitarism, systemic inflammatory response syndrome, gastritis, duodenitis, sarcoidosis, histiocytic necrotizing lymphadenitis (Kikuchi lymphadenitis), myositis, myocarditis, rhabdomyolysis, motor dysfunction, vasculitis, and myasthenic syndrome.
Infusion Reactions
OPDIVO can cause severe infusion reactions, which have been reported in <1.0% of patients in clinical trials. Discontinue OPDIVO in patients with Grade 3 or 4 infusion reactions. Interrupt or slow the rate of infusion in patients with Grade 1 or 2. In patients receiving OPDIVO monotherapy, infusion-related reactions occurred in 6.4% (127/1994) of patients. In patients receiving OPDIVO with YERVOY, infusion-related reactions occurred in 2.5% (10/407) of patients.
Complications of Allogeneic HSCT after OPDIVO
Complications, including fatal events, occurred in patients who received allogeneic HSCT after OPDIVO. Outcomes were evaluated in 17 patients from Checkmate 205 and 039, who underwent allogeneic HSCT after discontinuing OPDIVO (15 with reduced-intensity conditioning, 2 with myeloablative conditioning). Thirty-five percent (6/17) of patients died from complications of allogeneic HSCT after OPDIVO. Five deaths occurred in the setting of severe or refractory GVHD. Grade 3 or higher acute GVHD was reported in 29% (5/17) of patients. Hyperacute GVHD was reported in 20% (n=2) of patients. A steroid-requiring febrile syndrome, without an identified infectious cause, was reported in 35% (n=6) of patients. Two cases of encephalitis were reported: Grade 3 (n=1) lymphocytic encephalitis without an identified infectious cause, and Grade 3 (n=1) suspected viral encephalitis. Hepatic veno-occlusive disease (VOD) occurred in one patient, who received reduced-intensity conditioned allogeneic HSCT and died of GVHD and multi-organ failure. Other cases of hepatic VOD after reduced-intensity conditioned allogeneic HSCT have also been reported in patients with lymphoma who received a PD-1 receptor blocking antibody before transplantation. Cases of fatal hyperacute GVHD have also been reported. These complications may occur despite intervening therapy between PD-1 blockade and allogeneic HSCT.
Follow patients closely for early evidence of transplant-related complications such as hyperacute GVHD, severe (Grade 3 to 4) acute GVHD, steroid-requiring febrile syndrome, hepatic VOD, and other immune-mediated adverse reactions, and intervene promptly.
Embryo-Fetal Toxicity
Based on their mechanisms of action, OPDIVO and YERVOY can cause fetal harm when administered to a pregnant woman. Advise pregnant women of the potential risk to a fetus. Advise females of reproductive potential to use effective contraception during treatment with an OPDIVO- or YERVOY- containing regimen and for at least 5 months after the last dose of OPDIVO.
Lactation
It is not known whether OPDIVO or YERVOY is present in human milk. Because many drugs, including antibodies, are excreted in human milk and because of the potential for serious adverse reactions in nursing infants from an OPDIVO-containing regimen, advise women to discontinue breastfeeding during treatment. Advise women to discontinue nursing during treatment with YERVOY and for 3 months following the final dose.
Serious Adverse Reactions
In Checkmate 037, serious adverse reactions occurred in 41% of patients receiving OPDIVO (n=268). Grade 3 and 4 adverse reactions occurred in 42% of patients receiving OPDIVO . The most frequent Grade 3 and 4 adverse drug reactions reported in 2% to <5% of patients receiving OPDIVO were abdominal pain, hyponatremia, increased aspartate aminotransferase, and increased lipase. In Checkmate 066, serious adverse reactions occurred in 36% of patients receiving OPDIVO (n=206). Grade 3 and 4 adverse reactions occurred in 41% of patients receiving OPDIVO. The most frequent Grade 3 and 4 adverse reactions reported in ≥2% of patients receiving OPDIVO were gamma-glutamyltransferase increase (3.9%) and diarrhea (3.4%). In Checkmate 067, serious adverse reactions (73% and 37%), adverse reactions leading to permanent discontinuation (43% and 14%) or to dosing delays (55% and 28%), and Grade 3 or 4 adverse reactions (72% and 44%) all occurred more frequently in the OPDIVO plus YERVOY arm (n=313) relative to the OPDIVO arm (n=313). The most frequent (≥10%) serious adverse reactions in the OPDIVO plus YERVOY arm and the OPDIVO arm, respectively, were diarrhea (13% and 2.6%), colitis (10% and 1.6%), and pyrexia (10% and 0.6%). In Checkmate 017 and 057, serious adverse reactions occurred in 46% of patients receiving OPDIVO (n=418). The most frequent serious adverse reactions reported in at least 2% of patients receiving OPDIVO were pneumonia, pulmonary embolism, dyspnea, pyrexia, pleural effusion, pneumonitis, and respiratory failure. In Checkmate 025, serious adverse reactions occurred in 47% of patients receiving OPDIVO (n=406). The most frequent serious adverse reactions reported in ≥2% of patients were acute kidney injury, pleural effusion, pneumonia, diarrhea, and hypercalcemia. In Checkmate 205 and 039, adverse reactions leading to discontinuation occurred in 7% and dose delays due to adverse reactions occurred in 34% of patients (n=266). Serious adverse reactions occurred in 26% of patients. The most frequent serious adverse reactions reported in ≥1% of patients were pneumonia, infusion-related reaction, pyrexia, colitis or diarrhea, pleural effusion, pneumonitis, and rash. Eleven patients died from causes other than disease progression: 3 from adverse reactions within 30 days of the last OPDIVO dose, 2 from infection 8 to 9 months after completing OPDIVO, and 6 from complications of allogeneic HSCT. In Checkmate 141, serious adverse reactions occurred in 49% of patients receiving OPDIVO. The most frequent serious adverse reactions reported in at least 2% of patients receiving OPDIVO were pneumonia, dyspnea, respiratory failure, respiratory tract infection, and sepsis. In Checkmate 275, serious adverse reactions occurred in 54% of patients receiving OPDIVO (n=270). The most frequent serious adverse reactions reported in at least 2% of patients receiving OPDIVO were urinary tract infection, sepsis, diarrhea, small intestine obstruction, and general physical health deterioration.
Common Adverse Reactions
In Checkmate 037, the most common adverse reaction (≥20%) reported with OPDIVO (n=268) was rash (21%). In Checkmate 066, the most common adverse reactions (≥20%) reported with OPDIVO (n=206) vs dacarbazine (n=205) were fatigue (49% vs 39%), musculoskeletal pain (32% vs 25%), rash (28% vs 12%), and pruritus (23% vs 12%). In Checkmate 067, the most common (≥20%) adverse reactions in the OPDIVO plus YERVOY arm (n=313) were fatigue (59%), rash (53%), diarrhea (52%), nausea (40%), pyrexia (37%), vomiting (28%), and dyspnea (20%). The most common (≥20%) adverse reactions in the OPDIVO (n=313) arm were fatigue (53%), rash (40%), diarrhea (31%), and nausea (28%). In Checkmate 017 and 057, the most common adverse reactions (≥20%) in patients receiving OPDIVO (n=418) were fatigue, musculoskeletal pain, cough, dyspnea, and decreased appetite. In Checkmate 025, the most common adverse reactions (≥20%) reported in patients receiving OPDIVO (n=406) vs everolimus (n=397) were asthenic conditions (56% vs 57%), cough (34% vs 38%), nausea (28% vs 29%), rash (28% vs 36%), dyspnea (27% vs 31%), diarrhea (25% vs 32%), constipation (23% vs 18%), decreased appetite (23% vs 30%), back pain (21% vs 16%), and arthralgia (20% vs 14%). In Checkmate 205 and 039, the most common adverse reactions (≥20%) reported in patients receiving OPDIVO (n=266) were upper respiratory tract infection (44%), fatigue (39%), cough (36%), diarrhea (33%), pyrexia (29%), musculoskeletal pain (26%), rash (24%), nausea (20%) and pruritus (20%). In Checkmate 141, the most common adverse reactions (≥10%) in patients receiving OPDIVO were cough and dyspnea at a higher incidence than investigator’s choice. In Checkmate 275, the most common adverse reactions (≥ 20%) reported in patients receiving OPDIVO (n=270) were fatigue (46%), musculoskeletal pain (30%), nausea (22%), and decreased appetite (22%).. The most common adverse reactions (≥20%) in patients who received OPDIVO as a single agent were fatigue, rash, musculoskeletal pain, pruritus, diarrhea, nausea, asthenia, cough, dyspnea, constipation, decreased appetite, back pain, arthralgia, upper respiratory tract infection, pyrexia.
In a separate Phase 3 study of YERVOY 3 mg/kg, the most common adverse reactions (≥5%) in patients who received YERVOY at 3 mg/kg were fatigue (41%), diarrhea (32%), pruritus (31%), rash (29%), and colitis (8%).
Tuesday, August 15, 2017 4:30 pm EDT
PRINCETON, N.J.--(BUSINESS WIRE)--Bristol-Myers Squibb Company (NYSE: BMY) announced topline results today from the CheckMate -214 trial investigating Opdivo (nivolumab) in combination with Yervoy (ipilimumab) versus sunitinib in intermediate and poor-risk patients previously untreated advanced or metastatic renal cell carcinoma. The combination met the co-primary endpoint of objective response rate (ORR) and achieved a 41.6% ORR versus 26.5% for sunitinib. Median duration of response was not reached for the combination of Opdivo and Yervoy and was 18.17 months for sunitinib. While there was an improvement in progression-free survival (PFS) (HR=0.82, [95% CI 0.64 – 1.05]; stratified 2-sided p=0.03), it did not reach statistical significance. The median PFS was 11.56 months (95% CI 8.71 – 15.51) for the Opdivo and Yervoy combination versus 8.38 months (95% CI 7.03-10.81) for sunitinib, The study will continue as planned to allow the third co-primary endpoint of overall survival to mature. The tolerability profile observed in CheckMate-214 was consistent with that observed in previously reported studies of this dosing schedule.
“We are encouraged by the totality of the CheckMate-214 data. The overall response rate and durability of response favored the combination of Opdivo and Yervoy, and the trend for PFS supports the potential of the combination in intermediate and poor-risk advanced renal cell carcinoma, the most common type of kidney cancer. This is an important study in first-line renal cancer as these patients need new options,” said Vicki Goodman, M.D., development lead, Melanoma and Genitourinary Cancers, Bristol-Myers Squibb. “We look forward to presenting the full results from this study at an upcoming medical meeting.”
“Opdivo is now well established as standard of care in the treatment of second-line renal cell carcinoma,” said Goodman. “The company plans to share these important first-line data with regulatory authorities and we look forward to reporting overall survival when these data mature.”
About CheckMate -214
CheckMate -214 is a phase 3, randomized, open-label study evaluating the combination of Opdivo plus Yervoy versus sunitinib in patients with previously untreated advanced or metastatic renal cell carcinoma. Patients in the combination group received Opdivo 3 mg/kg plus Yervoy 1 mg/kg every 3 weeks for 4 doses followed by Opdivo 3 mg/kg every 2 weeks. Patients in the comparator group received sunitinib 50 mg once daily for 4 weeks, followed by 2 weeks off before continuation of treatment. Patients were treated until progression or unacceptable toxic effects. The primary endpoints of the trial are progression-free survival, overall survival and objective response rate in an intermediate to poor-risk patient population (approximately 75 percent of patients). The majority of alpha was allocated to overall survival. Safety is a secondary endpoint.
...
IMPORTANT SAFETY INFORMATION
WARNING: IMMUNE-MEDIATED ADVERSE REACTIONS
YERVOY can result in severe and fatal immune-mediated adverse reactions. These immune-mediated reactions may involve any organ system; however, the most common severe immune-mediated adverse reactions are enterocolitis, hepatitis, dermatitis (including toxic epidermal necrolysis), neuropathy, and endocrinopathy. The majority of these immune-mediated reactions initially manifested during treatment; however, a minority occurred weeks to months after discontinuation of YERVOY.
Assess patients for signs and symptoms of enterocolitis, dermatitis, neuropathy, and endocrinopathy and evaluate clinical chemistries including liver function tests (LFTs), adrenocorticotropic hormone (ACTH) level, and thyroid function tests at baseline and before each dose.
Permanently discontinue YERVOY and initiate systemic high-dose corticosteroid therapy for severe immune-mediated reactions.
Immune-Mediated Pneumonitis
OPDIVO can cause immune-mediated pneumonitis. Fatal cases have been reported. Monitor patients for signs with radiographic imaging and for symptoms of pneumonitis. Administer corticosteroids for Grade 2 or more severe pneumonitis. Permanently discontinue for Grade 3 or 4 and withhold until resolution for Grade 2. In patients receiving OPDIVO monotherapy, fatal cases of immune-mediated pneumonitis have occurred. Immune-mediated pneumonitis occurred in 3.1% (61/1994) of patients. In patients receiving OPDIVO with YERVOY, immune-mediated pneumonitis occurred in 6% (25/407) of patients.
In Checkmate 205 and 039, pneumonitis, including interstitial lung disease, occurred in 6.0% (16/266) of patients receiving OPDIVO. Immune-mediated pneumonitis occurred in 4.9% (13/266) of patients receiving OPDIVO: Grade 3 (n=1) and Grade 2 (n=12).
Immune-Mediated Colitis
OPDIVO can cause immune-mediated colitis. Monitor patients for signs and symptoms of colitis. Administer corticosteroids for Grade 2 (of more than 5 days duration), 3, or 4 colitis. Withhold OPDIVO monotherapy for Grade 2 or 3 and permanently discontinue for Grade 4 or recurrent colitis upon re-initiation of OPDIVO. When administered with YERVOY, withhold OPDIVO and YERVOY for Grade 2 and permanently discontinue for Grade 3 or 4 or recurrent colitis. In patients receiving OPDIVO monotherapy, immune-mediated colitis occurred in 2.9% (58/1994) of patients. In patients receiving OPDIVO with YERVOY, immune-mediated colitis occurred in 26% (107/407) of patients including three fatal cases.
In a separate Phase 3 study of YERVOY 3 mg/kg, severe, life-threatening, or fatal (diarrhea of ≥7 stools above baseline, fever, ileus, peritoneal signs; Grade 3-5) immune-mediated enterocolitis occurred in 34 (7%) patients. Across all YERVOY-treated patients in that study (n=511), 5 (1%) developed intestinal perforation, 4 (0.8%) died as a result of complications, and 26 (5%) were hospitalized for severe enterocolitis.
Immune-Mediated Hepatitis
OPDIVO can cause immune-mediated hepatitis. Monitor patients for abnormal liver tests prior to and periodically during treatment. Administer corticosteroids for Grade 2 or greater transaminase elevations. Withhold for Grade 2 and permanently discontinue for Grade 3 or 4 immune-mediated hepatitis. In patients receiving OPDIVO monotherapy, immune-mediated hepatitis occurred in 1.8% (35/1994) of patients. In patients receiving OPDIVO with YERVOY, immune-mediated hepatitis occurred in 13% (51/407) of patients.
In a separate Phase 3 study of YERVOY 3 mg/kg, severe, life-threatening, or fatal hepatotoxicity (AST or ALT elevations >5x the ULN or total bilirubin elevations >3x the ULN; Grade 3-5) occurred in 8 (2%) patients, with fatal hepatic failure in 0.2% and hospitalization in 0.4%.
Immune-Mediated Neuropathies
In a separate Phase 3 study of YERVOY 3 mg/kg, 1 case of fatal Guillain-Barré syndrome and 1 case of severe (Grade 3) peripheral motor neuropathy were reported.
Immune-Mediated Endocrinopathies
OPDIVO can cause immune-mediated hypophysitis, immune-mediated adrenal insufficiency, autoimmune thyroid disorders, and Type 1 diabetes mellitus. Monitor patients for signs and symptoms of hypophysitis, signs and symptoms of adrenal insufficiency, thyroid function prior to and periodically during treatment, and hyperglycemia. Administer hormone replacement as clinically indicated and corticosteroids for Grade 2 or greater hypophysitis. Withhold for Grade 2 or 3 and permanently discontinue for Grade 4 hypophysitis. Administer corticosteroids for Grade 3 or 4 adrenal insufficiency. Withhold for Grade 2 and permanently discontinue for Grade 3 or 4 adrenal insufficiency. Administer hormone-replacement therapy for hypothyroidism. Initiate medical management for control of hyperthyroidism. Withhold OPDIVO for Grade 3 and permanently discontinue for Grade 4 hyperglycemia.
In patients receiving OPDIVO monotherapy, hypophysitis occurred in 0.6% (12/1994) of patients. In patients receiving OPDIVO with YERVOY, hypophysitis occurred in 9% (36/407) of patients. In patients receiving OPDIVO monotherapy, adrenal insufficiency occurred in 1% (20/1994) of patients. In patients receiving OPDIVO with YERVOY, adrenal insufficiency occurred in 5% (21/407) of patients. In patients receiving OPDIVO monotherapy, hypothyroidism or thyroiditis resulting in hypothyroidism occurred in 9% (171/1994) of patients. Hyperthyroidism occurred in 2.7% (54/1994) of patients receiving OPDIVO monotherapy. In patients receiving OPDIVO with YERVOY, hypothyroidism or thyroiditis resulting in hypothyroidism occurred in 22% (89/407) of patients. Hyperthyroidism occurred in 8% (34/407) of patients receiving OPDIVO with YERVOY. In patients receiving OPDIVO monotherapy, diabetes occurred in 0.9% (17/1994) of patients. In patients receiving OPDIVO with YERVOY, diabetes occurred in 1.5% (6/407) of patients.
In a separate Phase 3 study of YERVOY 3 mg/kg, severe to life-threatening immune-mediated endocrinopathies (requiring hospitalization, urgent medical intervention, or interfering with activities of daily living; Grade 3-4) occurred in 9 (1.8%) patients. All 9 patients had hypopituitarism, and some had additional concomitant endocrinopathies such as adrenal insufficiency, hypogonadism, and hypothyroidism. 6 of the 9 patients were hospitalized for severe endocrinopathies.
Immune-Mediated Nephritis and Renal Dysfunction
OPDIVO can cause immune-mediated nephritis. Monitor patients for elevated serum creatinine prior to and periodically during treatment. Administer corticosteroids for Grades 2-4 increased serum creatinine. Withhold OPDIVO for Grade 2 or 3 and permanently discontinue for Grade 4 increased serum creatinine. In patients receiving OPDIVO monotherapy, immune-mediated nephritis and renal dysfunction occurred in 1.2% (23/1994) of patients. In patients receiving OPDIVO with YERVOY, immune-mediated nephritis and renal dysfunction occurred in 2.2% (9/407) of patients.
Immune-Mediated Skin Adverse Reactions and Dermatitis
OPDIVO can cause immune-mediated rash, including Stevens-Johnson syndrome (SJS) and toxic epidermal necrolysis (TEN), some cases with fatal outcome. Administer corticosteroids for Grade 3 or 4 rash. Withhold for Grade 3 and permanently discontinue for Grade 4 rash. For symptoms or signs of SJS or TEN, withhold OPDIVO and refer the patient for specialized care for assessment and treatment; if confirmed, permanently discontinue. In patients receiving OPDIVO monotherapy, immune-mediated rash occurred in 9% (171/1994) of patients. In patients receiving OPDIVO with YERVOY, immune-mediated rash occurred in 22.6% (92/407) of patients.
In a separate Phase 3 study of YERVOY 3 mg/kg, severe, life-threatening, or fatal immune-mediated dermatitis (eg, Stevens-Johnson syndrome, toxic epidermal necrolysis, or rash complicated by full thickness dermal ulceration, or necrotic, bullous, or hemorrhagic manifestations; Grade 3-5) occurred in 13 (2.5%) patients. 1 (0.2%) patient died as a result of toxic epidermal necrolysis. 1 additional patient required hospitalization for severe dermatitis.
Immune-Mediated Encephalitis
OPDIVO can cause immune-mediated encephalitis. Evaluation of patients with neurologic symptoms may include, but not be limited to, consultation with a neurologist, brain MRI, and lumbar puncture. Withhold OPDIVO in patients with new-onset moderate to severe neurologic signs or symptoms and evaluate to rule out other causes. If other etiologies are ruled out, administer corticosteroids and permanently discontinue OPDIVO for immune-mediated encephalitis. In patients receiving OPDIVO monotherapy, encephalitis occurred in 0.2% (3/1994) of patients. Fatal limbic encephalitis occurred in one patient after 7.2 months of exposure despite discontinuation of OPDIVO and administration of corticosteroids. Encephalitis occurred in one patient receiving OPDIVO with YERVOY (0.2%) after 1.7 months of exposure.
Other Immune-Mediated Adverse Reactions
Based on the severity of adverse reaction, permanently discontinue or withhold treatment, administer high-dose corticosteroids, and, if appropriate, initiate hormone-replacement therapy. Across clinical trials of OPDIVO the following clinically significant immune-mediated adverse reactions occurred in <1.0% of patients receiving OPDIVO: uveitis, iritis, pancreatitis, facial and abducens nerve paresis, demyelination, polymyalgia rheumatica, autoimmune neuropathy, Guillain-Barré syndrome, hypopituitarism, systemic inflammatory response syndrome, gastritis, duodenitis, sarcoidosis, histiocytic necrotizing lymphadenitis (Kikuchi lymphadenitis), myositis, myocarditis, rhabdomyolysis, motor dysfunction, vasculitis, and myasthenic syndrome.
Infusion Reactions
OPDIVO can cause severe infusion reactions, which have been reported in <1.0% of patients in clinical trials. Discontinue OPDIVO in patients with Grade 3 or 4 infusion reactions. Interrupt or slow the rate of infusion in patients with Grade 1 or 2. In patients receiving OPDIVO monotherapy, infusion-related reactions occurred in 6.4% (127/1994) of patients. In patients receiving OPDIVO with YERVOY, infusion-related reactions occurred in 2.5% (10/407) of patients.
Complications of Allogeneic HSCT after OPDIVO
Complications, including fatal events, occurred in patients who received allogeneic HSCT after OPDIVO. Outcomes were evaluated in 17 patients from Checkmate 205 and 039, who underwent allogeneic HSCT after discontinuing OPDIVO (15 with reduced-intensity conditioning, 2 with myeloablative conditioning). Thirty-five percent (6/17) of patients died from complications of allogeneic HSCT after OPDIVO. Five deaths occurred in the setting of severe or refractory GVHD. Grade 3 or higher acute GVHD was reported in 29% (5/17) of patients. Hyperacute GVHD was reported in 20% (n=2) of patients. A steroid-requiring febrile syndrome, without an identified infectious cause, was reported in 35% (n=6) of patients. Two cases of encephalitis were reported: Grade 3 (n=1) lymphocytic encephalitis without an identified infectious cause, and Grade 3 (n=1) suspected viral encephalitis. Hepatic veno-occlusive disease (VOD) occurred in one patient, who received reduced-intensity conditioned allogeneic HSCT and died of GVHD and multi-organ failure. Other cases of hepatic VOD after reduced-intensity conditioned allogeneic HSCT have also been reported in patients with lymphoma who received a PD-1 receptor blocking antibody before transplantation. Cases of fatal hyperacute GVHD have also been reported. These complications may occur despite intervening therapy between PD-1 blockade and allogeneic HSCT.
Follow patients closely for early evidence of transplant-related complications such as hyperacute GVHD, severe (Grade 3 to 4) acute GVHD, steroid-requiring febrile syndrome, hepatic VOD, and other immune-mediated adverse reactions, and intervene promptly.
Embryo-Fetal Toxicity
Based on their mechanisms of action, OPDIVO and YERVOY can cause fetal harm when administered to a pregnant woman. Advise pregnant women of the potential risk to a fetus. Advise females of reproductive potential to use effective contraception during treatment with an OPDIVO- or YERVOY- containing regimen and for at least 5 months after the last dose of OPDIVO.
Lactation
It is not known whether OPDIVO or YERVOY is present in human milk. Because many drugs, including antibodies, are excreted in human milk and because of the potential for serious adverse reactions in nursing infants from an OPDIVO-containing regimen, advise women to discontinue breastfeeding during treatment. Advise women to discontinue nursing during treatment with YERVOY and for 3 months following the final dose.
Serious Adverse Reactions
In Checkmate 037, serious adverse reactions occurred in 41% of patients receiving OPDIVO (n=268). Grade 3 and 4 adverse reactions occurred in 42% of patients receiving OPDIVO . The most frequent Grade 3 and 4 adverse drug reactions reported in 2% to <5% of patients receiving OPDIVO were abdominal pain, hyponatremia, increased aspartate aminotransferase, and increased lipase. In Checkmate 066, serious adverse reactions occurred in 36% of patients receiving OPDIVO (n=206). Grade 3 and 4 adverse reactions occurred in 41% of patients receiving OPDIVO. The most frequent Grade 3 and 4 adverse reactions reported in ≥2% of patients receiving OPDIVO were gamma-glutamyltransferase increase (3.9%) and diarrhea (3.4%). In Checkmate 067, serious adverse reactions (73% and 37%), adverse reactions leading to permanent discontinuation (43% and 14%) or to dosing delays (55% and 28%), and Grade 3 or 4 adverse reactions (72% and 44%) all occurred more frequently in the OPDIVO plus YERVOY arm (n=313) relative to the OPDIVO arm (n=313). The most frequent (≥10%) serious adverse reactions in the OPDIVO plus YERVOY arm and the OPDIVO arm, respectively, were diarrhea (13% and 2.6%), colitis (10% and 1.6%), and pyrexia (10% and 0.6%). In Checkmate 017 and 057, serious adverse reactions occurred in 46% of patients receiving OPDIVO (n=418). The most frequent serious adverse reactions reported in at least 2% of patients receiving OPDIVO were pneumonia, pulmonary embolism, dyspnea, pyrexia, pleural effusion, pneumonitis, and respiratory failure. In Checkmate 025, serious adverse reactions occurred in 47% of patients receiving OPDIVO (n=406). The most frequent serious adverse reactions reported in ≥2% of patients were acute kidney injury, pleural effusion, pneumonia, diarrhea, and hypercalcemia. In Checkmate 205 and 039, adverse reactions leading to discontinuation occurred in 7% and dose delays due to adverse reactions occurred in 34% of patients (n=266). Serious adverse reactions occurred in 26% of patients. The most frequent serious adverse reactions reported in ≥1% of patients were pneumonia, infusion-related reaction, pyrexia, colitis or diarrhea, pleural effusion, pneumonitis, and rash. Eleven patients died from causes other than disease progression: 3 from adverse reactions within 30 days of the last OPDIVO dose, 2 from infection 8 to 9 months after completing OPDIVO, and 6 from complications of allogeneic HSCT. In Checkmate 141, serious adverse reactions occurred in 49% of patients receiving OPDIVO. The most frequent serious adverse reactions reported in at least 2% of patients receiving OPDIVO were pneumonia, dyspnea, respiratory failure, respiratory tract infection, and sepsis. In Checkmate 275, serious adverse reactions occurred in 54% of patients receiving OPDIVO (n=270). The most frequent serious adverse reactions reported in at least 2% of patients receiving OPDIVO were urinary tract infection, sepsis, diarrhea, small intestine obstruction, and general physical health deterioration.
Common Adverse Reactions
In Checkmate 037, the most common adverse reaction (≥20%) reported with OPDIVO (n=268) was rash (21%). In Checkmate 066, the most common adverse reactions (≥20%) reported with OPDIVO (n=206) vs dacarbazine (n=205) were fatigue (49% vs 39%), musculoskeletal pain (32% vs 25%), rash (28% vs 12%), and pruritus (23% vs 12%). In Checkmate 067, the most common (≥20%) adverse reactions in the OPDIVO plus YERVOY arm (n=313) were fatigue (59%), rash (53%), diarrhea (52%), nausea (40%), pyrexia (37%), vomiting (28%), and dyspnea (20%). The most common (≥20%) adverse reactions in the OPDIVO (n=313) arm were fatigue (53%), rash (40%), diarrhea (31%), and nausea (28%). In Checkmate 017 and 057, the most common adverse reactions (≥20%) in patients receiving OPDIVO (n=418) were fatigue, musculoskeletal pain, cough, dyspnea, and decreased appetite. In Checkmate 025, the most common adverse reactions (≥20%) reported in patients receiving OPDIVO (n=406) vs everolimus (n=397) were asthenic conditions (56% vs 57%), cough (34% vs 38%), nausea (28% vs 29%), rash (28% vs 36%), dyspnea (27% vs 31%), diarrhea (25% vs 32%), constipation (23% vs 18%), decreased appetite (23% vs 30%), back pain (21% vs 16%), and arthralgia (20% vs 14%). In Checkmate 205 and 039, the most common adverse reactions (≥20%) reported in patients receiving OPDIVO (n=266) were upper respiratory tract infection (44%), fatigue (39%), cough (36%), diarrhea (33%), pyrexia (29%), musculoskeletal pain (26%), rash (24%), nausea (20%) and pruritus (20%). In Checkmate 141, the most common adverse reactions (≥10%) in patients receiving OPDIVO were cough and dyspnea at a higher incidence than investigator’s choice. In Checkmate 275, the most common adverse reactions (≥ 20%) reported in patients receiving OPDIVO (n=270) were fatigue (46%), musculoskeletal pain (30%), nausea (22%), and decreased appetite (22%).. The most common adverse reactions (≥20%) in patients who received OPDIVO as a single agent were fatigue, rash, musculoskeletal pain, pruritus, diarrhea, nausea, asthenia, cough, dyspnea, constipation, decreased appetite, back pain, arthralgia, upper respiratory tract infection, pyrexia.
In a separate Phase 3 study of YERVOY 3 mg/kg, the most common adverse reactions (≥5%) in patients who received YERVOY at 3 mg/kg were fatigue (41%), diarrhea (32%), pruritus (31%), rash (29%), and colitis (8%).




















02.05.24 · wO Chartvergleich · Ansys |
02.05.24 · Sharedeals · CytomX Therapeutics |
12.03.24 · wO Chartvergleich · Blackbaud (Old) |