



Diskussion zu CytoSorbents Corporation (Seite 168)
eröffnet am 20.05.09 17:22:57 von
neuester Beitrag 30.04.24 22:46:00 von
neuester Beitrag 30.04.24 22:46:00 von
Beiträge: 4.238
ID: 1.150.520
ID: 1.150.520
Aufrufe heute: 53
Gesamt: 689.849
Gesamt: 689.849
Aktive User: 0
ISIN: US23283X2062 · WKN: A12GDU
0,8730
EUR
+8,04 %
+0,0650 EUR
Letzter Kurs 21:57:09 Quotrix Düsseldorf
Neuigkeiten
02.05.24 · globenewswire |
26.04.24 · globenewswire |
17.04.24 · globenewswire |
14.03.24 · globenewswire |
Werte aus der Branche Gesundheitswesen
| Wertpapier | Kurs | Perf. % |
|---|---|---|
| 5,8750 | +187,99 | |
| 0,7400 | +36,63 | |
| 0,7700 | +28,76 | |
| 3,5100 | +27,64 | |
| 3,8450 | +22,45 |
| Wertpapier | Kurs | Perf. % |
|---|---|---|
| 1,4550 | -14,91 | |
| 3,5000 | -19,54 | |
| 2,4900 | -26,55 | |
| 2,5900 | -32,11 | |
| 2,4100 | -51,51 |
Beitrag zu dieser Diskussion schreiben
Antwort auf Beitrag Nr.: 61.732.756 von NoamX am 21.10.19 09:30:54Das wäre sicher ideal, aber ist es letztlich nicht egal? Solange die herausgefilterten Substanzen nicht zu Problemen führen wäre es vielleicht sogar Zeitverschwendung diesen Punkt zu optimieren...nach einer Blutspende bildet der Körper ja auch die entnommenen Substanzen rasch wieder nach. Ich kann am "Schrotflintenansatz" erst mal nichts wirklich schlimmes erkennen.
Zitat von NoamX: Aber es liest auch etwas so, dass Cytosrob ein Schrotflintenansatz ist, der möglicherweise zu viel aus dem Blut filtert. Wenn nur 3 der ausgefilterten 39 Moleküle schädlich sind, sollte man dann nicht versuchen, nur diese heruszufiltern, und die anderen 36 in Blut zu belassen?
Antwort auf Beitrag Nr.: 61.732.756 von NoamX am 21.10.19 09:30:54Was die nähere Zukunft anbelangt, bin ich auch der Meinung, dass die Anwendung im Bereich "Entfernung von Blutverdünnern aus dem Blut" richtig Schubkraft bringen könnte, denn die Kombination aus medizinischem und wirtschaftlichem Nutzen macht die Entscheidung für den Cytosorb-Adsorber schlicht und ergreifend rational.
Hier sollte man übrigens nicht vergessen, dass auch ohne eine FDA-Zulassung das Potenzial groß genug ist, um ein enormes Wachstum zu ermöglichen. Das Problem ist doch eher, dass die Argumente für den Einsatz der Adsorber bislang in den Augen der Anwender noch nicht stark genug waren, um zu einer breiten Anwendung zu führen. Aus meiner Sicht ändert sich dies aber immer mehr. Tatsächlich ist es so, dass ich inzwischen keine grundsätzlichen Zweifel mehr an der Wirksamkeit des Adsorbers hege. Trotzdem sind noch Wissenslücken zu schließen.
Insofern nehme ich an, dass die besagte Studie über die Wirtschaftlichkeit der Cytosorb-Adsorber in dieser Indikation hier tatsächlich kurzfristig zu einem Nachfragesog führen könnte.
Bei der Sepsis verhält es sich aus meiner Sicht ein wenig anders. Hier hat das Management von Cytosorbents offensichtlich vor ein paar Jahren Abstand davon genommen, direkt eine Sepsis-Studie durchzuführen. Das Problem war nach meinem Verständnis, dass die Erfolgsausichten einer Studie fraglich waren. Der Grund dafür waren einerseits die große Heterogenität der Patienten und deren Erkrankungen und andererseits die schlechte Prognostizierbarkeit der Krankheitsverläufe, nicht zuletzt auch aufgrund des komplexen Krankheitsbildes und des unvollständigen medizinischen Wissens. Hinzu kam die Anforderung seitens der FDA, einen Überlebensvorteil zu belegen.
Möglicherweise war die Entscheidung, zunächt auf eine Sepsis-Studie in den USA zu verzichten, die größte bisherige Leistung des Managements!
Nachdem aber die Erfahrung mit dem Cytosorb-Adsorber und das medizinische Wissen über die Sepsis ständig angewachsen sind (auch durch solche Studien wie die aus Ulm), ist man womöglich in absehbarer Zeit dazu in der Lage, eine erfolgversprechende Sepsis-Studie zu konzipieren, um die gewünschte FDA-Zulassung zu erhalten.
Hier sollte man übrigens nicht vergessen, dass auch ohne eine FDA-Zulassung das Potenzial groß genug ist, um ein enormes Wachstum zu ermöglichen. Das Problem ist doch eher, dass die Argumente für den Einsatz der Adsorber bislang in den Augen der Anwender noch nicht stark genug waren, um zu einer breiten Anwendung zu führen. Aus meiner Sicht ändert sich dies aber immer mehr. Tatsächlich ist es so, dass ich inzwischen keine grundsätzlichen Zweifel mehr an der Wirksamkeit des Adsorbers hege. Trotzdem sind noch Wissenslücken zu schließen.
Insofern nehme ich an, dass die besagte Studie über die Wirtschaftlichkeit der Cytosorb-Adsorber in dieser Indikation hier tatsächlich kurzfristig zu einem Nachfragesog führen könnte.
Bei der Sepsis verhält es sich aus meiner Sicht ein wenig anders. Hier hat das Management von Cytosorbents offensichtlich vor ein paar Jahren Abstand davon genommen, direkt eine Sepsis-Studie durchzuführen. Das Problem war nach meinem Verständnis, dass die Erfolgsausichten einer Studie fraglich waren. Der Grund dafür waren einerseits die große Heterogenität der Patienten und deren Erkrankungen und andererseits die schlechte Prognostizierbarkeit der Krankheitsverläufe, nicht zuletzt auch aufgrund des komplexen Krankheitsbildes und des unvollständigen medizinischen Wissens. Hinzu kam die Anforderung seitens der FDA, einen Überlebensvorteil zu belegen.
Möglicherweise war die Entscheidung, zunächt auf eine Sepsis-Studie in den USA zu verzichten, die größte bisherige Leistung des Managements!
Nachdem aber die Erfahrung mit dem Cytosorb-Adsorber und das medizinische Wissen über die Sepsis ständig angewachsen sind (auch durch solche Studien wie die aus Ulm), ist man womöglich in absehbarer Zeit dazu in der Lage, eine erfolgversprechende Sepsis-Studie zu konzipieren, um die gewünschte FDA-Zulassung zu erhalten.
Antwort auf Beitrag Nr.: 61.731.529 von Der kleine Aktienfreund am 21.10.19 01:03:48Aber es liest auch etwas so, dass Cytosrob ein Schrotflintenansatz ist, der möglicherweise zu viel aus dem Blut filtert. Wenn nur 3 der ausgefilterten 39 Moleküle schädlich sind, sollte man dann nicht versuchen, nur diese heruszufiltern, und die anderen 36 in Blut zu belassen?
Trotzdem: Die Dichte an Studien, die Cytosorb eine Wirksamkeit in verschiedenen Anwendungsfällen attestieren, ist mittlerweile beeindruckend.
Ich könnte mir aber vorstellen, dass die Studie zur Kostenreduktion möglicherweise kurzfristig bedeutender ist. Bei dieser Konstellation haben alle Beteiligte Krankenhäuser, Ärzte, Kostenträger und Cytosorbents gemeinsame Interessen, was die Zulassungs hoffentlich beschleunigt.
Trotzdem: Die Dichte an Studien, die Cytosorb eine Wirksamkeit in verschiedenen Anwendungsfällen attestieren, ist mittlerweile beeindruckend.
Ich könnte mir aber vorstellen, dass die Studie zur Kostenreduktion möglicherweise kurzfristig bedeutender ist. Bei dieser Konstellation haben alle Beteiligte Krankenhäuser, Ärzte, Kostenträger und Cytosorbents gemeinsame Interessen, was die Zulassungs hoffentlich beschleunigt.
Antwort auf Beitrag Nr.: 61.723.961 von MisterMarket72 am 19.10.19 09:15:32Die Studie, von der du hier berichtet hast, ist möglicherweise sehr bedeutend. Wenn es den Ulmer Forschern tatsächlich gelungen ist, die Schlüsselfaktoren für den Verlauf der Sepsis zu identifizieren, dann wachsen die Chancen auf eine erfolgreiche Sepsis-Studie, da sich so womöglich die Patienten anhand dieser Kriterien auswählen lassen.
Hier ist ein Beitrag zu der Veröffentlichung aus dem Yahoo-Board von einem Teilnehmer namens hofno2003, der mir bisher durch seine fundierten Kommentare positiv aufgefallen ist:
########################################################################################
Groundbreaking paper with Cytosorb published in Nature.com: detailed analysis of adsorbed molecular compounds
triggering the hemodynamic instability of blood vessels and subsequent multi organ failure
########################################################################################
Why is this paper groundbreaking? It clarifies the mechanism of action concerning the reversal and prevention of organ damage - which is the root cause for death in the setting of a septic shock. The authors clearly demonstrate, by analyzing the CytoSorb adsorbed mixture of molecules (cytokines, chemokines, pamps, damps, activated complement....), that a very specific and small fraction of these adsorbed and in the blood circulating molecular entities are responsible for the impairment of the circulatory system. This small fraction of circulating and by CytoSorb adsorbed molecules is composed of an till now unidentified protein highly enriched with nucleic acids (free DNA and RNA released by cell damage or maybe intentionally sheded by cells to trap pathogens) in the size range of 15 kilodalton.
The authors tested 39 fractions of molecular material adsorbed from whole blood by CytoSorb by washing this out of the used adsorbers - but just 3 of these 39 fraction had an adverse effect on endothelial function (proper function of the blood vessel lining), while all others had not. The adverse effects are cell death (apoptosis), reduced ATP content (means reduced cellular metabolism) and inhibition of proliferation (means that the endothel will not be repaired after injury).
These findings also explain, why all other trials with other interventions in a sepsis setting finally fail - because the root cause for endothelial failure and patients death is just a small but very specific subset of all released DAMPS and PAMPS and cytokines and LPS and myoglobin/hemoglobin, ...... This does not mean that it is not beneficial to remove these additional signals - because it is also good to interrupt the inflammatory cascade which is of course moderated by cytokines, but it demonstrates that the final mechanism leading to death of a patient by the impairment of the blood vessel system and resulting multi organ failure during sepsis is now more specifically identified and can be managed by CytoSorb. GROUNDBRAKING NEWS for me and the medical community. You can find the paper by Google using the term: “Bioassay for endothelial Damage Mediators Retrieved by Hemoadsorption”. Yahoo didn’t allow to post a link – sorry.
Hier ist ein Beitrag zu der Veröffentlichung aus dem Yahoo-Board von einem Teilnehmer namens hofno2003, der mir bisher durch seine fundierten Kommentare positiv aufgefallen ist:
########################################################################################
Groundbreaking paper with Cytosorb published in Nature.com: detailed analysis of adsorbed molecular compounds
triggering the hemodynamic instability of blood vessels and subsequent multi organ failure
########################################################################################
Why is this paper groundbreaking? It clarifies the mechanism of action concerning the reversal and prevention of organ damage - which is the root cause for death in the setting of a septic shock. The authors clearly demonstrate, by analyzing the CytoSorb adsorbed mixture of molecules (cytokines, chemokines, pamps, damps, activated complement....), that a very specific and small fraction of these adsorbed and in the blood circulating molecular entities are responsible for the impairment of the circulatory system. This small fraction of circulating and by CytoSorb adsorbed molecules is composed of an till now unidentified protein highly enriched with nucleic acids (free DNA and RNA released by cell damage or maybe intentionally sheded by cells to trap pathogens) in the size range of 15 kilodalton.
The authors tested 39 fractions of molecular material adsorbed from whole blood by CytoSorb by washing this out of the used adsorbers - but just 3 of these 39 fraction had an adverse effect on endothelial function (proper function of the blood vessel lining), while all others had not. The adverse effects are cell death (apoptosis), reduced ATP content (means reduced cellular metabolism) and inhibition of proliferation (means that the endothel will not be repaired after injury).
These findings also explain, why all other trials with other interventions in a sepsis setting finally fail - because the root cause for endothelial failure and patients death is just a small but very specific subset of all released DAMPS and PAMPS and cytokines and LPS and myoglobin/hemoglobin, ...... This does not mean that it is not beneficial to remove these additional signals - because it is also good to interrupt the inflammatory cascade which is of course moderated by cytokines, but it demonstrates that the final mechanism leading to death of a patient by the impairment of the blood vessel system and resulting multi organ failure during sepsis is now more specifically identified and can be managed by CytoSorb. GROUNDBRAKING NEWS for me and the medical community. You can find the paper by Google using the term: “Bioassay for endothelial Damage Mediators Retrieved by Hemoadsorption”. Yahoo didn’t allow to post a link – sorry.
Uni Ulm
Spannender Artikel bei nature.com (PDF-Downloadlink: https://www.nature.com/articles/s41598-019-50517-1.pdf) vom 10.10.2019. Die Uniklinik Ulm hat in Sachen Sepsis und Cytosorb schwer geforscht.The study design was as follows: Patients were enrolled to our study when admitted to the ICU within 48 hours after sepsis onset and presenting with high plasma interleukin (IL)-6 concentrations (>500 pg/ml) and/or kid-ney failure. When a patient was enrolled and planned to be treated with CytoSorb hemoadsorption therapy, one blood sample was taken before the treatment. During the treatment, infection markers were routinely checked. After 24 hours of treatment, another blood sample was taken. The CytoSorb adsorber cartridge was immediately processed (see below). Cytokine measurements and leukocyte antigen expression analysis were performed before and after CytoSorb hemoadsorption treatment.We here report representative results on the biochemical preparation of a single hemoadsorption device per-formed in a 76-year-old female patient after surgery for an abdominal aneurysm through Crawford access and clamping of visceral and renal arteries. Sepsis was diagnosed, according to Singer and colleagues (2016), by the presence of catecholamine-dependent septic shock, hemodynamics and a lactate concentration >2 mg/dl follow-ing the Sepsis 3 criteria on day 3 after surgery (catecholamines were administered at 0.4 μg/kg Body Weight (BW)/min, lactate was 4.9 mg/dl), and inflammatory variables were highly elevated, including C-reactive protein (CRP): 307.6 mg/l; procalcitonin (PCT): 5.68 μg/l; IL-6: 4944 pg/ml; and IL-8: 308 pg/ml; as was lactate dehydrogenase (266 U/l). The patient benefitted from CytoSorb treatment in that the catecholamine dosage was decreased to 0.05 μg/kgBW/min and most of the other inflammatory parameters declined, including CRP (235.5 mg/l), PCT (4.3 μg/l), IL-6 (107.4 pg/ml) and IL-8 (63.6 pg/ml), whereas lactate remained elevated (5.2 μg/l).
Leider bin ich nicht vom Fach und auch nicht wirklich schlau genug, aber wenn ich die Studie richtig verstehe, hat man dann 39 verschiedene Proteine aus so einem Adsorber isolieren und vier davon als zellaktiv identifizieren können.
In summary, four different protein fractions were classified as “active” (F10–F12, F24) for their significant inhibitory effect on mEC proliferation. The remaining fractions had no effect on mEC proliferation and did not increase cell death.
Es waren wohl auch nicht einheitlich immer 39 verschiedene Protein-„Fractions“ sondern auch mal 46:
The same procedure was performed with hemoadsorbed material from two other patients, one of whom benefitted from CytoSorb treatment (data not shown). A total of 46 protein fractions were obtained from the responding patient, two of which: F26-F27 impaired mEC proliferation and increased cell death. By con-trast, none of the 44 protein fractions obtained from the hemoadsorbed material of the non-responding patient affected mEC confluency or viability (data not shown). The reasons for these differences are likely related to the individual elution profile of the column fractionation and await further investigations.
Und was soll das alles?
Die Ulmer meinen erkannt zu haben, dass der Adsorber bei Sepsis hilft, ohne dass das bislang wirklich konkret erklärbar ist oder war. Um der Sache auf den Grund zu gehen, schraubt man nun einen im Sepsis-Kontext benutzten Adsorber auf, untersucht, welches Zeug der so eingesammelt hat und schaut, was von dem Zeug „zellaktiv“ ist bzw. Zellen umbringt. Macht Sinn, oder? Noch mal: was wirklich 100% genau bei Sepsis los ist, weiß bis heute keiner. Der Ansatz der Ulmer hier ist für meine Begriffe richtig gut, logisch und stringent und sowas alles.
In summary, the molecular entities fractionated from CytoSorb adsorbers of a patient with septic shock had a major impact on mEC confluency, cell layer integrity, proliferation, ATP contents mEC apoptosis. These features may contribute to the clinical observations of perfusion deficiency and organ failure in patients with septic shock.
Zitieren wir noch ein bisschen, um zu zeigen, wie komplex der ganze Kram ist:
Discussion
A major pathology in septic shock occurs by endothelial cell damage, which contributes to organ failure. The pathology related to coagulation factors has been excellently reviewed by Opal and van der Poll23. Essentially, sol-uble factors and activated immune cells contribute to alterations in coagulation and cause increased endothelial permeability. William Aird drewed the following conclusion: “…it would be difficult to identify a single com-ponent whose therapeutic modulation will short-circuit the sepsis cascade and improve outcome34”, our results provide further evidence for multiple protein entities involved in different pathways to cause sepsis-related endothelial dysfunction. In vivo, additional effects are expected to occur by leukocytes interacting with mEC in an inflammatory environment. As reviewed in an excellent manuscript, the co-activation of both cytoplas-mic toll-like receptror-(TLR)4 – and TLR3-guided non-canonical inflammasome activation is a likely target to attenuate severity in septic shock models35. One reason was the fulminant beneficial effect by CytoSorb hemoad-sorption to restore endothelial function and restrict septic shock through a major reduction of catecholamine treatment within 24 hours. We first addressed inflammatory mediators removed by CytoSorb treatment, similar to previous34 investigations focusing on inflammatory cytokines (IL-6) and coagulation factors9,10, and then frac-tionated the proteins adsorbed to a CytoSorb column by classic peptide biochemistry. An unbiased approach was followed using a novel bioassay with brain-derived mEC. A total of 39 CytoSorb-derived fractions were tested by long-term video microscopy using an IncuCyteZOOM device. This assay has the advantage of being able to simultaneously analyze9,10 cell proliferation, death and morphology36. Protein fractions F10–F12 and F24 were identified as having a major effect on the integrity of endothelial-cell layers and mEC viability, proliferation, ATP content and cell death-related mechanisms, including apoptosis. We are currently attempting to identify indi-vidual protein fractions affecting mEC from hemoadsorbed material of two additional patients as well as protein fractions pooled from eight other CytoSorb columns. These results will help us identify the protein fractions that affect mEC viability and identify their contents (cf. Fig. 7). In future experiments, we will focus on the identification of the 15 kDa protein species found in F10–F12
Schon noch ein bisschen Nebel und tausend Nebenfaktoren. Sei’s drum: die Ulmer konstatieren, dass das Ding funktioniert – am Warum wird eben noch gearbeitet:
In summary, the current work describes a mEC-based bioassay to study blood-derived mediators, which were efficiently eliminated by CytoSorb hemoadsorption treatment and may explain rapid resolution from states of septic shock after CytoSorb treatment.
Trading Spotlight
Kostenersparnis durch Adsorber-Einsatz im Ticagrelor-Kontext in UK bestätigt.
Das ganze man bei Springer nachlesen (hochangesehen und selektiv in der Artikel-Auswahl): https://link.springer.com/content/pdf/10.1007%2Fs41669-019-0…
"Results
In emergent cardiac surgery, intraoperative removal of ticagrelor using CytoSorb was less costly (£12,933 vs. £16,874) and more effective (0.06201vs. 0.06091 quality-adjusted life-years) than cardiac surgery without physiologic clear-ance of ticagrelor over a 30-day time horizon. For urgent cardiac surgery, the use of CytoSorb was less costly than any of the three comparators—delaying surgery for natural washout without adjunctive therapy, adjunctive therapy with short-acting antiplatelet agents, or adjunctive therapy with low-molecular-weight heparin. Results from the PSAs showed that CytoSorb has a high probability of being cost saving (99% in emergent cardiac surgery and 53–77% in urgent cardiac surgery, depend-ing on the comparators). Cost savings derive from fewer transfusions of blood products and re-thoracotomies, and shorter stay in the hospital/intensive care unit.
Conclusions
The implementation of CytoSorb as an intraoperative intervention for patients receiving ticagrelor undergo-ing emergent or urgent cardiac surgery is a cost-saving strategy, yielding improvement in perioperative and postoperative outcomes and decreased health resource use."
Das ganze man bei Springer nachlesen (hochangesehen und selektiv in der Artikel-Auswahl): https://link.springer.com/content/pdf/10.1007%2Fs41669-019-0…
"... therefore it was a dominant strategy compared with the usual standard of care where emergent surgery is performed without waiting for physiologic clearance of ticagrelor. "
Gestern war die Präsentation im Rahmen der "The MicroCap Rodeo Investor Conference" und der Vortrag und die Präsentation sind online.
"Forecast CytoSorbents 2020: Faster Growth Ahead"
"We believe 2020 will be a year of strong growth and...."
Die aktuellen Ergebnisse diverser Studien (u.a. Maasstad Ziekenhuis Holland, St. Georg Krankhaus Hamburg) wurden eingebaut.
https://cytosorbents.com/wp-content/uploads/2019/10/CytoSorb…
https://www.webcaster4.com/Webcast/Page/2134/31830
"Forecast CytoSorbents 2020: Faster Growth Ahead"
"We believe 2020 will be a year of strong growth and...."
Die aktuellen Ergebnisse diverser Studien (u.a. Maasstad Ziekenhuis Holland, St. Georg Krankhaus Hamburg) wurden eingebaut.
https://cytosorbents.com/wp-content/uploads/2019/10/CytoSorb…
https://www.webcaster4.com/Webcast/Page/2134/31830
Antwort auf Beitrag Nr.: 61.698.352 von Aliberto am 15.10.19 19:33:25
Wenn man auf die Beschriftung rechts achtet, müsste die Stunde 0 "at the cessation of CPB" sein. Dass 0 der Start der OP sein soll, passt auch nicht so gut zum Titel des Charts ("... AFTER Surgery"). Sei's drum. Wir müssen ja nicht einer Meinung sein.
Meine "second hit" Theorie findet meiner Meinung nach auch in folgendem Chart Futter:
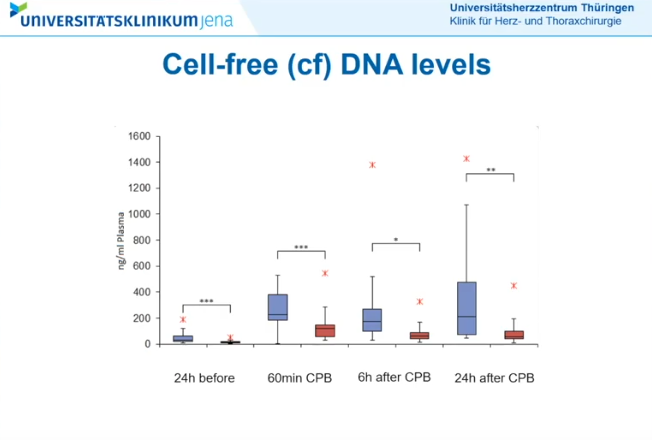
6h after CPB sieht alles halbwegs kontrolliert aus. 24h after CPB vergleichsweise nicht mehr.
Zitat von Aliberto: "Die Stunde 0 markiert nach meinem Verständnis das Ende der OP." => Nein, die "Stunde 0" markiert den Beginn der OP bei einer IE und den Anschluss des Patienten an die Herz-Lungen-Maschine (CPB !).
Wenn man auf die Beschriftung rechts achtet, müsste die Stunde 0 "at the cessation of CPB" sein. Dass 0 der Start der OP sein soll, passt auch nicht so gut zum Titel des Charts ("... AFTER Surgery"). Sei's drum. Wir müssen ja nicht einer Meinung sein.
Meine "second hit" Theorie findet meiner Meinung nach auch in folgendem Chart Futter:

6h after CPB sieht alles halbwegs kontrolliert aus. 24h after CPB vergleichsweise nicht mehr.
Antwort auf Beitrag Nr.: 61.698.295 von NoamX am 15.10.19 19:28:45Bitte noch mal den IL-6-Chart anschauen. Findest du, dass dein Kommentar auch für IL-6 passt? Ich nicht.
Und bitte nicht falsch verstehen: ich mach drei Purzelbäumen, wenn ich unrecht habe und REMOVE tolle Ergebnisse bringt.
Und bitte nicht falsch verstehen: ich mach drei Purzelbäumen, wenn ich unrecht habe und REMOVE tolle Ergebnisse bringt.
Antwort auf Beitrag Nr.: 61.697.122 von MisterMarket72 am 15.10.19 17:16:00"Die Stunde 0 markiert nach meinem Verständnis das Ende der OP." => Nein, die "Stunde 0" markiert den Beginn der OP bei einer IE und den Anschluss des Patienten an die Herz-Lungen-Maschine (CPB !).
Prof. Dr. med. Torsten Doenst sagt ja auch ganz klar, es passiert etwas bei Endocarditis-Patienten während der OP mit Anschluss an die Herz-Lungen-Maschine. Und je länger die Dauer der OP und der Anschluss an die Herz-Lungen-Maschine ist, je höher sind gewisse Zytokinwerte.
Die finanzierende Stelle will jetzt den klaren Nachweis haben (two-arm randomized-controlled group sequential (Pocock) design for assessing superiority and safety), dass der Filter diese Zytokine eliminiert und dass die positiven Effekte (primäre und sekundäre Endpunkte) ganz eindeutig aus der Elimination durch den Filter stammen.
Wenn der Filter jetzt im REMOVE-Trial auch noch 24 Stunden oder 48 Stunden nach der OP eingesetzt werden würde, könnte die Reduktion der Zytokine und Verbesserung u.a. des SOFA-Scores ja auch durch die eigentliche OP eingetreten sein und nichts mit dem Filter zu tun haben.
Du schaust auf die falschen Grafiken ! Schau auf die Grafiken Min. 4.37 ff Surgery / Operation und dann auf die Zytokinwerte während der Phase des CPB.
Prof. Dr. med. Torsten Doenst sagt ja auch ganz klar, es passiert etwas bei Endocarditis-Patienten während der OP mit Anschluss an die Herz-Lungen-Maschine. Und je länger die Dauer der OP und der Anschluss an die Herz-Lungen-Maschine ist, je höher sind gewisse Zytokinwerte.
Die finanzierende Stelle will jetzt den klaren Nachweis haben (two-arm randomized-controlled group sequential (Pocock) design for assessing superiority and safety), dass der Filter diese Zytokine eliminiert und dass die positiven Effekte (primäre und sekundäre Endpunkte) ganz eindeutig aus der Elimination durch den Filter stammen.
Wenn der Filter jetzt im REMOVE-Trial auch noch 24 Stunden oder 48 Stunden nach der OP eingesetzt werden würde, könnte die Reduktion der Zytokine und Verbesserung u.a. des SOFA-Scores ja auch durch die eigentliche OP eingetreten sein und nichts mit dem Filter zu tun haben.
Du schaust auf die falschen Grafiken ! Schau auf die Grafiken Min. 4.37 ff Surgery / Operation und dann auf die Zytokinwerte während der Phase des CPB.



















